
By Stephanie Prendergast, MPT, Cofounder, PHRC Pasadena
Urinary leaking during sneezing and coughing is common. Constipation affects millions of people. Irritative bladder symptoms plague women at multiple points in their life for a number of reasons, and bother men too. If one stops to think about orthopedic surgeries for broken ankles and shoulder dysfunction, why isn’t pelvic floor physical and occupational therapy part of the standard of care after all pelvic surgeries?
If you fall into any of the categories listed above you should consider an evaluation with a pelvic floor physical and occupational therapists. When people find us on their own their first question is often “why didn’t my doctor tell me?.” The fact is almost all medical schools lack information on various pelvic pain and pelvic floor disorders and therefore most physicians do not know that pelvic floor physical and occupational therapy exists and can help their suffering patients!
Let’s explain these six reasons that no one thinks to call a PT about:
Urinary leaking
Leaking urine is a symptom. Millions of people leak, and therefore this treatable symptom gets chalked up to part of the aging process or because you just had a baby. The reality is leaking is a sign of pelvic floor dysfunction and it should be addressed
Constipation
Constipation also plagues millions of people. In order for humans to evacuate stool the pelvic floor muscles have to autonomically and voluntarily relax. If the muscles are not functioning properly constipation can occur.
Bladder irritability
Irritative bladder symptoms can be miserable. Did you know pelvic floor dysfunction can mimic the symptoms of urinary tract infections? One should always undergo cultures to rule out infection. If the cultures are negative, consider an evaluation with a pelvic floor physical and occupational therapists.
Postpartum
All postpartum women should see a physical and occupational therapists. Pregnancy, labor and delivery are exceptional physiological situations and women need to rehabilitate afterwards.
Gender affirming surgery
Gender affirming surgeries essentially reorganize the pelvis. We are here to help people recover and live their best life!
Pelvic Surgery
Pelvic surgeries such as prostatectomy, pelvic organ prolapse repair, and hysterectomy are major surgeries that influence how your pelvic floor functions. Pelvic physical and occupational therapy should be offered prior to surgery to help with recovery and after surgery for rehabilitation.
While all of these scenarios are common, they are not normal and a sign of pelvic floor dysfunction. A good pelvic evaluation will help you learn what your individual impairments are and how to help.
Common reasons for these symptoms and pelvic floor dysfunction exist.
In general, most symptomatic people fall into one or a combination of these categories:
- Tight and painful pelvic floor and girdle muscles.
- Weak pelvic floor and girdle muscles.
- Tight and weak pelvic floor muscles.
- Coordination issues of the pelvic floor and girdle muscles.
- Presence of a diastasis recti.
- Nerve or muscle involvement after surgery or childbirth.
The pelvic floor muscles are an integral part of our core, playing crucial roles in urinary, bowel, and sexual function, as well as contributing to our overall comfort. Seemingly minor symptoms, such as leaking when sneezing, indicate that these muscles are not functioning optimally. It is important to seek evaluation and treatment early to prevent the development of more significant and disruptive symptoms.
While general categories of impairment exist, people with the same symptoms often have different underlying causes. This is why we do not use protocols, a one-size-fits-all approach is more like one-size-fits none. We pride ourselves on helping our patients best understand their bodies and help them restore their pelvic health!
How Do We Do Pelvic Floor Physical and Occupational Therapy?
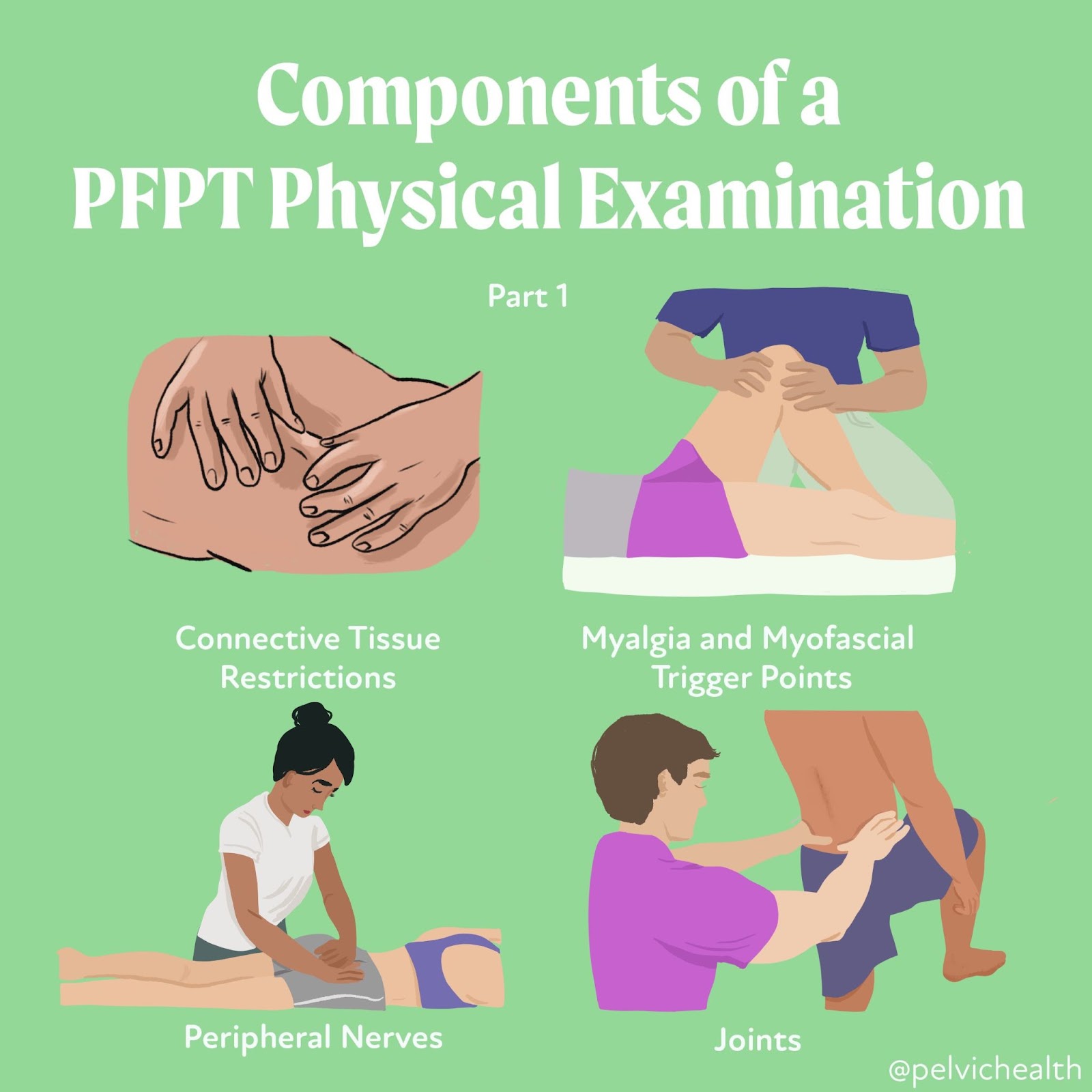
At PHRC we focus our in-person visits on things our patients cannot do for themselves. This may include manual therapy such as myofascial release and connective tissue manipulation, joint manipulation and neuromuscular re-education. We also provide impairment-specific home exercises to lengthen, strengthen, or help to improve neuromuscular control. We establish short term goals that are typically expected to be achieved in six to eight visits. We also establish long term goals which are tied to someone’s desired functional outcome, such as not leaking, having easy bowel movements, and urinating no more than six to eight times in a 24 hour period with distress or urgency. People should not have to think about their bladders!
People often ask if they have to do their exercises and home program forever. The answer is it depends, sometimes yes and sometimes no.
Have questions? So do many other people. Please see our FAQ list below and message us with your comments and questions!
Frequently Asked Questions
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor therapy?
Pelvic floor therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapists need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
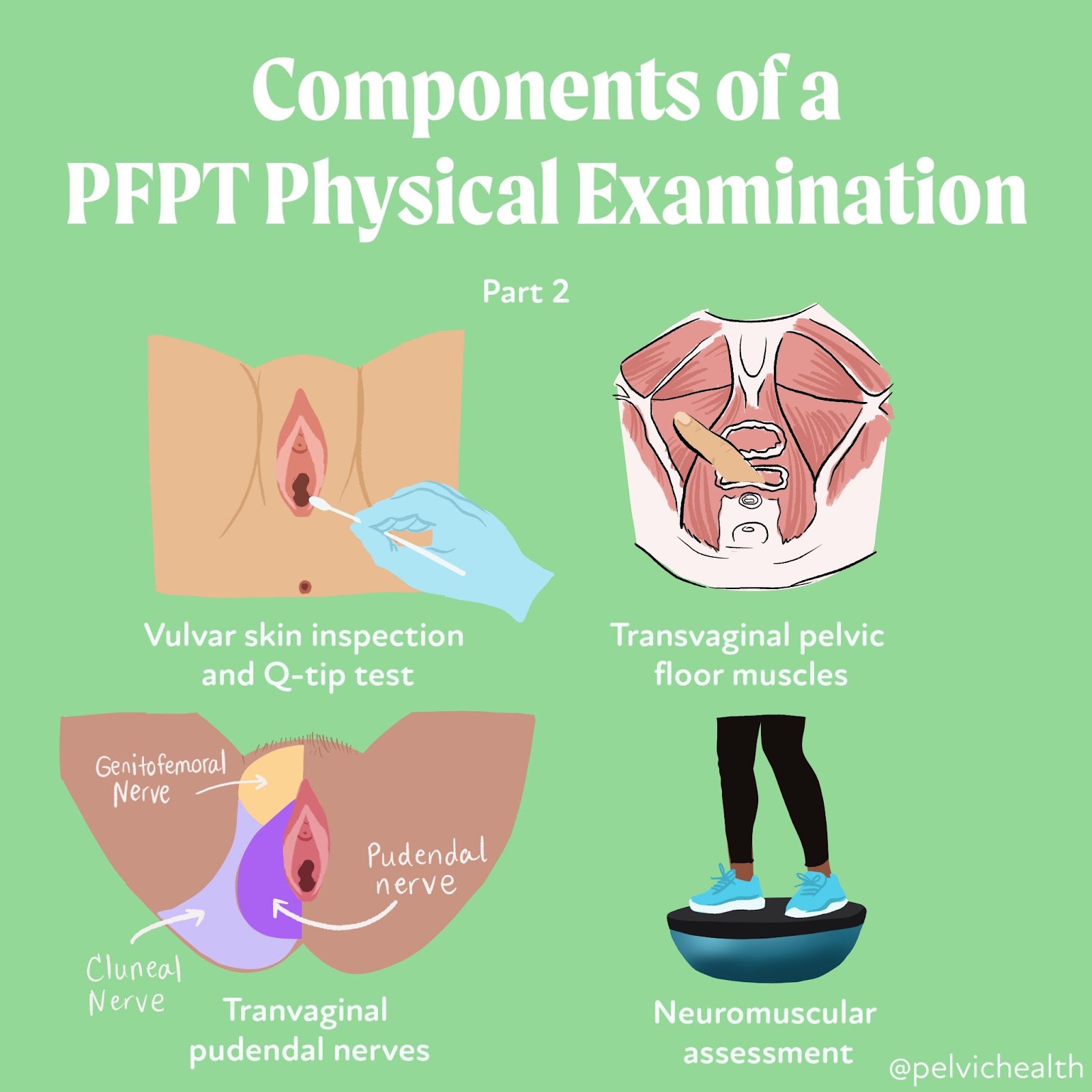
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The pelvic floor physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for three months to a year.
______________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Did you know we opened our 11th location in Columbus, OH? Now scheduling new patients- call (510) 922-9836 to book!
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.