
By Katie Hunter, DPT
Drop, push, bulge, squeeze. These words are used regularly when talking about pelvic floor function but what do they actually mean?
We often talk about how the pelvic floor muscles become dysfunctional and can cause daily symptoms of pelvic pain, bladder and bowel urgency and frequency, incontinence, prolapse, and sexual dysfunction. Today, I would like to lay out how the pelvic floor muscles normally function and clear up some of the confusing terminology practitioners use. I encourage those that are new to the pelvic floor muscles anatomy to first read Shannon’s blog, Your pelvic floor: what is it good for?
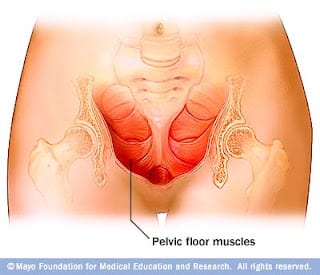

The main functions of the pelvic floor muscles are sphincteric, supportive, and sexual. These muscles close the bottom of the pelvis to support all of our organs and keep the openings closed to prevent leaking, they contract when we achieve climax or orgasm, and they have the ability to relax in order to empty our bladders and bowels. Therefore, these muscles are necessary for our most essential functions.
In order to provide enough support for our pelvic organs, the pelvic floor muscles need to effectively counteract intra-abdominal pressures. When we exert ourselves, such as during coughing, sneezing, laughing, and lifting, a large amount of force is placed on the body and abdomen. If our pelvic floor muscles do not function appropriately, we may leak or feel pressure in the pelvis when participating in these activities.
Two things that most influence how well our pelvic floor muscles function are breathing and posture. Our trunks are supported by our “core” muscles which include the diaphragm (the “roof”), the abdominal muscles, the pelvic floor muscles (the “floor”), and the spinal column and back muscles. The core muscles work in synergy throughout the day to support our trunk, spine, and pelvis; preventing injury and pain.

There should be a natural ebb-and-flow that occurs between all of these muscles and our breath. When we take an inhale, the dome-shaped diaphragm muscle flattens moving our organs down in the abdominal cavity. In order to avoid squashing our organs, our pelvic floor and abdominal muscles lengthen and expand to allow the organs to move down. As we exhale, the diaphragm lifts and the pelvic floor and abdominal muscles return to their resting position.
A common error we see with our patients is the habit of holding one’s breath. People often hold their breath during strenuous activity, in times of stress, or during bowel movements which can lead to a wide variety of pelvic floor dysfunctions. This is why pelvic floor physical and occupational therapistss focus so much on coordinating the breath with muscle control.

How we sit, stand, walk, and move will affect our pelvic floor muscles. Posture and the pelvic floor muscles have a direct affect on each other, described as an interdependence.6 For ideal standing posture, physical and occupational therapistss use a plumbline through the body to assess a person’s posture.
Carriere and Feldt describe the plumbline of ideal standing posture as follows:6
- Slightly anterior to the lateral malleolus
- Slightly anterior to the axis of the knee joint
- Slightly anterior to the axis of the hip joint
- Through the bodies of the lumbar vertebrae
- Through the shoulder joint
- Through the bodies of the cervical vertebrae
- Through the external auditory meatus
- Slightly posterior to the apex of the coronal suture
Many factors can affect our posture. Lifestyle and habits, pain, tight muscles, weak muscles, weight, and mood. If your hamstring muscles are tight, they can cause your pelvis to tilt backwards so that you are in a slouched position when you sit which can lead to tight pelvic floor muscles and pelvic floor dysfunction. If your abdominal muscles are weak, they cannot support your abdomen and you may stand with a sway back which can lead to lower back pain and pelvic pain. Becoming aware of healthy, symmetrical posture will help in optimizing the function of the pelvic floor.

Along with our voluntary functions of the pelvic floor muscles throughout the day, these muscles also have a large reflexive role. The urethral and anal sphincters are activated by reflexes to maintain bladder and bowel control. These reflexes are elicited by stimuli to the skin, pelvic organ distension, pain, and intra-abdominal pressure changes. Notably, pelvic floor muscle tone automatically increases with a sudden increase in intra-abdominal pressure (i.e. coughing, sneezing) and with pain to the pelvic organs and pelvic region.5 Neuromuscular re-education can help to strengthen and improve these reflexes to improve bowel and bladder control.

Physical therapists who specialize in the treatment of pelvic floor muscles aim to normalize muscle tone and length, motor control, coordination, strength and endurance. This is done by a combination of posture training, breathwork, exercises, lifestyle changes, and manual therapy to balance the core muscles and improve their function. The following are common terms we as physical and occupational therapistss use for pelvic floor muscle training:
- Isolated pelvic floor (PF) muscle contractions (aka Kegels): isolated activation of the pelvic floor muscles. There are two types of isolated PF muscle exercises.
- Quick flicks: focusing on recruitment of the urogenital triangle to close the urethra, these exercises help to gain strength in the “fast twitch” muscle fibers of the pelvic floor to improve control of the bladder and reduce leakage with coughing, sneezing, and laughing.
- Quick kegels: this is an isolated contraction of the pelvic floor muscles throughout the entire range of motion including recruitment of the levator ani muscles. We focus on full tissue excursion including complete relaxation between contractions. They can be coordinated with our breath on the exhale to train the synergy of the diaphragm and pelvic floor.
- Slow (endurance) kegels: similar to the quick kegels, but this exercise aims to train our slow-twitch muscle fibers. This is where you hold the pelvic floor contraction to build endurance in the muscle for activities such as prolonged standing, carrying items, and walking. Slow kegels can be coordinated with or without our breath.
- Abdominal brace: isolated activation of the transverse abdominis muscle which works to stabilize the spine and pelvis during activity. On the exhale, this is a drawing of your belly button back towards your spine and “hip” bones towards each other. Research shows that people are less likely to suffer from lower back pain when this muscle is actively working throughout the day.1-3
- Pelvic brace: co-activation of the transverse abdominis and pelvic floor muscles for lower back and pelvic stability. The pelvic brace helps to support our joints and organs to minimize injury/leaking/prolapse. Performed on the exhale, activating the two muscle groups together can reduce pain and improve bladder/bowel control; focus on performing a pelvic brace with exertion (i.e. getting in and out of bed, standing from a chair, pushing/pulling, lifting, etc.) can also help reduce stress incontinence.
- Diaphragmatic breathing: Because of the way the pelvic floor muscles and diaphragm are shaped and work together, when we practice diaphragmatic breathing, this encourages the pelvic floor muscles to relax. Diaphragmatic breathing is deep belly breathing that focuses on activation of the diaphragm for the greatest lung ventilation and muscle relaxation. As we inhale, the diaphragm flattens and the pelvic floor muscles lengthen.
- Pelvic floor muscle bulge: described by Rhonda Kotarinos as reciprocal inhibition which is defined as “relaxation of an agonist muscle during contraction of the antagonist muscle.”4 I teach activation of the abdominal muscles while facilitating relaxation of the pelvic floor muscles with the cues, “belly big, belly hard while blooming a flower with the pelvic floor muscles” during an exhalation. A PFM bulge can help to initiate a bowel movement followed by PF drops and relaxation.
- Pelvic floor muscle relaxation: also called a pelvic floor “drop,” this is a voluntary relaxation of the pelvic floor muscles where the muscles lengthen down towards the feet. Imagery assists in achieving pelvic floor relaxation by imagining blooming a flower or spreading the sit bones. This is also termed as the ante-Kegel or reverse Kegel.
A pelvic floor muscle training program is not one-size fits all. We recommend being evaluated by a pelvic floor specialist who can prescribe a combination of these exercises in order to improve your daily function that is specific to your individual needs.
References:
- Kang, J. Jeong D. Choi, H. (2016). Effect of exhalation exercise on trunk muscle activity and oswestry disability index of patients with chronic low back pain. J Phys Ther Sci. 28(6). 1738-42.
- N. Hooper, T. Dedrick, G. Brismee, J. Sizer, P. (2017). The effect of current low back pain on volitional preemptive abdominal activation during a loaded forward reach activity. Physical Medicine and Rehab Journal. 9(2). 127-135.
- Watson, T. McPherson, S. Fleeman, S. (2011). Ultrasound measurement of transverse abdominis during loaded, functional tasks in asymptomatic individuals: rater reliability. Physical Medicine and Rehab Journal. 3. 697-705.
- FitzGerald, M. Kotarinos, R. (2003). Rehabilitation of the short pelvic floor. II: treatment of the patient with the short pelvic floor. Int Urogynecol J. 14. 269-275.
- K. Bo, B. Berghmans, S. Morkved, M. Van Kampen. (2007). Evidence-based physical and occupational therapy for the pelvic floor. 19-20.
- B. Carriere, C.M. Feldt. (2006). The pelvic floor. 68-81.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
Who in atlanta has really learned and teaching what you talk about. There are so many quote pelvic floor physical specialist. How do I check gradientals to confirm they are really trained in that field. I have pelvic floor dyssynergia and paradoxical puborectalis contractions some just say Anismus
Thank you
ann broussard [email protected]
Hi Ann,
Please use the link below to find a pelvic floor physical therapist.
https://pelvicguru.com/2016/02/13/find-a-pelvic-health-professional/
Regards,
Admin
LOVE this article Katie! Thank you so much for sharing!
This was a very informative article with wonderful explanations. Thank you so much!
Thank you for sharing the Knowledge
I am a physical therapist
Great article! Feeling sooo optimistic ❤❤❤❤