
By Shannon Pacella, DPT, PHRC Lexington
Medical marijuana. You’ve probably heard of it. You’ve maybe even used it. But what you might not know about is the tug-of-war going on between researchers and lawmakers, and how this impacts the ability of this stigmatized substance to be studied – potentially missing out on an alternative treatment option for a multitude of health issues, including pelvic pain.
Let’s start with a little background history. The two main cannabinoids (compounds) from the marijuana plant that are of medical interest to researchers are THC and CBD. CBD is a cannabinoid that is considered non-psychoactive (although it may reduce anxiety), while THC does have psychoactive properties.1 In 1970, the United States Congress placed marijuana in Schedule I of the Controlled Substances Act (CSA).2 According to the United States Drug Enforcement Administration (DEA), “Schedule I drugs, substances, or chemicals are defined as drugs with no currently accepted medical use and a high potential for abuse.”3 Sounds pretty harsh, right? Well fast-forward to present day where currently 25 states plus Washington D.C. have legalized the use of medical marijuana, and 16 other states have legalized non-psychoactive medical cannabis (CBD extract).2 Each state has specific parameters regarding the amount and forms that are considered legal.

The huge disparity between each state’s rules and regulations makes medical marijuana a complicated substance to not only obtain for personal use, but also for researchers looking to further expand what is currently known about marijuana and it’s potential benefits. On August 11, 2016, the U.S. DEA declined to move marijuana from Schedule I to a less-restrictive schedule under the CSA, but has begun the process of allowing more research to be done. The U.S. DEA has created a policy to expand the amount of DEA-registered marijuana manufacturers in order to adequately supply researchers.3
Even though there is tight regulation on the ability to conduct research regarding medical marijuana, the limited findings have yielded great results. THC has been proven to increase appetite and reduce nausea, so the FDA has approved THC-based medications for these purposes (dronabinol and nabilone).1 There have been a number of studies revealing the powerful effects that medical marijuana can have on pain as well. A patient survey of medical cannabis users (for chronic pain) revealed, “average pre-treatment pain on a zero to ten scale was 7.8, whereas average post-treatment pain was 2.8, giving a reported average improvement of 5 points. This translates to a 64% average relative decrease in pain. Others reported therapeutic benefits included relief from stress/anxiety (50% of respondents), relief of insomnia (45%), improved appetite (12%), decreased nausea (10%), increased focus/concentration (9%), and relief from depression (7%).”4 A number of studies have also revealed that medical marijuana can reduce neuropathic pain (something that many people with pelvic pain, including pudendal neuralgia may encounter).5,6,7 Another study looked specifically at men with chronic prostatitis/chronic pelvic pain syndrome who used marijuana.8 The men self-reported in person (clinic) and online. “38.6% of clinic and 75% of online respondents reported that it improved their symptoms. Most of the respondents reported that cannabis improved their mood, pain, muscle spasms, and sleep.”8 You can learn more about male pelvic pain disorders here. Cannabis is also listed as a therapeutic pharmacological treatment for endometriosis, which you can learn more about here.
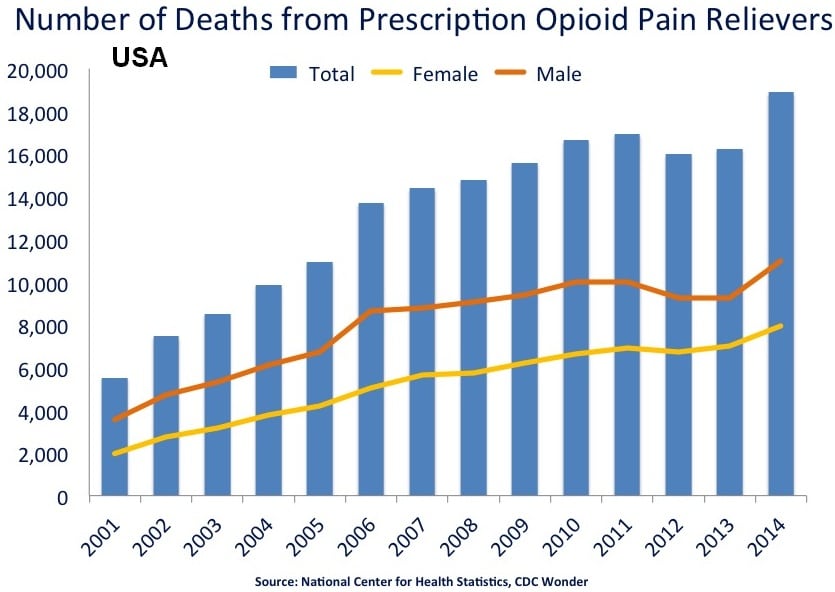
Another major topic is the relationship between medical marijuana and opioid use. The Centers for Disease Control (CDC) has presented that prescription opioid overdoses have killed more than 165,000 Americans between 1999 and 2014.9 On the other hand, the CDC has reported zero deaths from marijuana overdose ever. Interestingly enough, a study published in 2014 revealed an intriguing trend: from 1999 – 2010, states that allowed medical marijuana use had an average of almost 25% fewer opioid overdose deaths each year than states where cannabis remained illegal.10 Migrating away from prescription opioid use in favor of medical marijuana for pain relief may be the way of the future.
On top of all of these great discoveries is another surprise. All of the 2016 presidential candidates can agree on something: the support of medical marijuana and the need to continue to conduct research on it. Hillary Clinton stated in an interview with Boston’s WBZ radio, “I do think on the federal level we need to remove marijuana from the Schedule I of drugs, move it to Schedule II, which will permit it to be the basis for medical research because it’s important that we learn as much as possible. And since it was a Schedule I drug we haven’t done that research. A lot of experts in the field are telling me we’ve got to learn a lot more.”11 Similarly, in an interview with Bill O’Reilly, Donald Trump said, “I do want to see what the medical effects are. I have to see what the medical effects are and, by the way — medical marijuana, medical? I’m in favor of it a hundred percent.”11
This recent push towards allowing and encouraging medical marijuana use and research will open the door to many more possibilities in alternative treatment options for a variety of medical conditions including chronic pain and neuropathic pain.
This topic is now finally being openly discussed by many medical professionals, including at the International Pelvic Pain Society conference. While attending this conference, I heard Dr. Allan Frankel give a lecture discussing utilizing cannabis for managing pain, anxiety, and sleep. To hear him summarize this presentation, click here (you can skip to 26:30). I’m interested to hear your thoughts and opinions on medical marijuana – what do you think about it? Any personal experiences with using medical marijuana for pelvic pain? You are welcome to share below in the comments!
References:
- National Institute on Drug Abuse. Drug facts: is marijuana medicine? https://www.drugabuse.gov/publications/drugfacts/marijuana-medicine
- http://medicalmarijuana.procon.org/
- United States Drug Enforcement Administration. https://www.dea.gov/
- Webb CW, Webb SM. Therapeutic Benefits of Cannabis: A Patient Survey. Hawai’i Journal of Medicine & Public Health. 2014;73(4):109-111.
- Wilsey B, Marcotte T, Deutsch R, Gouaux B, Sakai S, Donaghe H. Low-dose vaporized cannabis significantly improves neuropathic pain. J Pain. 2013;14(2):136-48.
- Ware MA, Wang T, Shapiro S, et al. Smoked cannabis for chronic neuropathic pain: a randomized controlled trial. CMAJ. 2010;182(14):694-701.
- Wilsey B, Marcotte T, Tsodikov A, et al. A randomized, placebo-controlled, crossover trial of cannabis cigarettes in neuropathic pain. J Pain. 2008 Jun;9(6):506-21.
- Tripp DA, Nickel JC, Katz L, Krsmanovic A, Ware MA, Santor D. A survey of cannabis (marijuana) use and self-reported benefit in men with chronic prostatitis/chronic pelvic pain syndrome. Canadian Urological Association Journal. 2014;8(11-12):901-905.
- Centers for Disease Control and Prevention. http://www.cdc.gov/drugoverdose/data/overdose.html
- Bachhuber MA, Saloner B, Cunningham CO, Barry CL. Medical cannabis laws and opioid analgesic overdose mortality in the United States, 1999-2010. JAMA Intern Med. 2014;174(10):1668-1673.
- Marijuana Policy Project. Where do they stand on marijuana policy? https://www.mpp.org/2016-presidential-candidates/
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
I’m a medical marijuana patient and daily user for about 4 years. I’ve had pelvic floor problems for a around a year. Specifically a tight pelvic floor. Marijuana, while helpful for the anxiety and stress that come with the condition, actually seems to tighten my pelvic floor up more and increases my symptoms (specifically the urgency and frequency), a few other people in forums have reported similar experiences. I’m working on stopping because of this and wouldn’t recommend marijuana to most people with a tight pelvic floor.
Author Shannon Pacella says:
Thank you for sharing your experience regarding marijuana use and pelvic and urinary dysfunction. Medical marijuana, just like other more traditional types of medications may affect people differently. There are many different types of medical marijuana (containing different ratios of CBD and THC), which can alter what types of symptoms it may help with. Dr. Allan Frankel, whom is discussed at the end of my blog post, is currently doing research regarding the different ratios of cannabinoids and how they may affect people differently. Hopefully with the push for more research on medical marijuana, we can get more evidence discussing the relationship between different types of marijuana and it’s affect on the pelvic floor and pelvic pain. Regarding your urinary urgency/frequency symptoms and tight pelvic floor, you might consider seeing a pelvic floor physical therapist for an evaluation, if you have not already done so.
Thank you again for sharing your experience.
-Shannon
I’ve had vulvodynia for many years now, and, although vaping cannabis does help me with my insomnia, anxiety and other bodily pain, I have found it aggravates my pelvic pain, which, to say the least, is very aggravating! 😉 I am also considering weening off, but I am wondering first if taking cannabis in other ways (oils, edibles, tinctures) might take care of the problem (i.e., perhaps the vape smoke is the aggravating factor) or if there are specific strains that are best for pelvic pain (I also seem to have developed interstitial cystitis and possible IBS). Any thoughts would be helpful- thanks!
Author Shannon Pacella says:
Hi Ilsa,
If you live in a state where medical cannabis is legal, I would suggest talking with a physician who grants medical cannabis cards/prescriptions. Dr. Allan Frankel, whom I mentioned in my blog post, has some good resources and information regarding the best ways to use medical cannabis to treat specific conditions. You may find this post from him about medical cannabis and interstitial cystitis helpful: http://www.greenbridgemed.com/interstitial-cystitis-inflamed-bladder-and-cannabidiol/
I would also suggest getting an evaluation from a pelvic floor physical therapist who can help to address your pelvic pain, interstitial cystitis and possible IBS related symptoms.
If I had to guess that’s the THC. My pelvic/bladder area hated it. I found a brand that is pure CBD, and then had no problems.
Hi Shannon,
I am 49 years old and have been suffering from chronic pelvic pain and nerve damage for 12 years. I have been taking maximum levels of opiods that can be prescribed for the past 5 years and taking opiods for more than 11 years. Last week my doctor discussed possibly trying medical marijuana to help with this debilitating pain/condition. I have been reading what I can online about the “benefits” of medical marijuana. My concerns/fears of this include withdrawals from opiods, fear of getting high from the marijuana as when I previously tried smoking marijuana as a teenager it made me extremely paranoid, not actually getting any pain relief and possible adverse side effects of this.
What would you recommend as a starting dosage based on what I described above? And what would you recommend to help with my fears and concerns?
Thank you for your article.
Author Shannon Pacella says:
Hi Parry,
The two main cannabinoids (compounds) from the marijuana plant are THC and CBD. CBD is a cannabinoid that is considered non-psychoactive (although it may reduce anxiety), while THC does have psychoactive properties. I would suggest talking with the physician who mentioned trialing the medical marijuana (cannabis) in regards to the starting dosage and the ratio/amount of THC and CBD in the particular type of medical cannabis you may try.
I would also suggest getting an evaluation from a pelvic floor physical therapist who can help to address your chronic pelvic pain.
I have been battling chronic pelvic pain /PN for almost two years. I medicate at night with 20mg cannabis/coconut oil capsules. Any high is slept off. I have also found that cannabis/coconut oil suppositories (used vaginally or rectally) work exceptionally well in relaxing the pelvic floor muscles with no psychoactive effects. They can be used during the day and at night. Cannabis is not a one size fits all and one really needs to spend time researching what works best for them.
I am a 55 year old male, whom five years ago began presenting with a urologic/defecation dilemma.
To this day, drs have been unable to diagnose why, and none of their medicines are helping with pain or function; (exception being Tamsulosin to help relax the urethra sphincter).
I read about how cannabis might help, and it did. I’ve been medicating myself in the evening with a small amount, that has helped immensely with the pain associated with the disability of being able to do #2 normally, and contrary to others with pelvic disorders, med marijuana actually decreases the bloating and relaxes my lower quadrant.
Rob
Shirley, what formulation of cannabis suppository are you using-THC, or CBD and THC? Where do you get them? I have never seen them in AZ. I have been using Valium suppositories for my pelvic floor dysfunction but it makes me sleepy and would rather try cannabis since it works so well for me with very little side effects.
Shannon,
I have been using medical cannabis for about a year for my pelvic pain and it is amazing. I prefer the CBD since it does not have the psychoactive effects, does not make me sleepy, is much cheaper ($40/bottle), and you do not need a medical card to purchase it. For more moderate pain the 2:1 CBD:THC oral tincture ($100/bottle) is what I have been using and it is incredible. It starts working in 15 minutes and the pain is tolerable or sometimes even gone within 30 minutes. The only side effect I have is sleepiness. When I told my surgeon about it she suggested I continue to use it since it would help my pelvic floor dysfunction/nerve pain, and it does. Thanks for doing this piece. I really think many patients could benefit from cannabis use for their pelvic pain.