
Menopause encompasses more than just hot flashes, night sweats, and mood swings. Despite being a common phase affecting roughly half of the population, menopause is often misunderstood, both by the public and many healthcare providers. This gap in knowledge can lead to unnecessary suffering, as many individuals are not fully informed about effective treatments.
Perimenopause, the transitional phase leading up to menopause, typically begins in a person’s 40s, with menopause itself usually occurring in the early 50s. While systemic symptoms like hot flashes and mood changes are well-known, many people also experience less obvious but equally impactful genitourinary symptoms. These can include painful intercourse, urinary urgency, frequent urination, leakage, burning sensations, recurrent vaginal and urinary tract infections, and vaginal dryness. Collectively, these symptoms are part of the Genitourinary Syndrome of Menopause (GSM). Additionally, many women experience pelvic floor dysfunction, which affects nearly 50% of women by their 50s and can overlap with GSM symptoms.
While systemic hormonal therapy is commonly used to manage menopause symptoms, it may not address the specific needs of those experiencing GSM. The North American Menopause Society recommends the use of vaginal estrogen as an effective treatment for alleviating GSM symptoms and improving quality of life.
Menopause encompasses more than just hot flashes, night sweats, and mood swings. Despite being a common phase affecting roughly half of the population, menopause is often misunderstood, both by the public and many healthcare providers. This gap in knowledge can lead to unnecessary suffering, as many individuals are not fully informed about effective treatments.
Perimenopause, the transitional phase leading up to menopause, typically begins in a person’s 40s, with menopause itself usually occurring in the early 50s. While systemic symptoms like hot flashes and mood changes are well-known, many people also experience less obvious but equally impactful genitourinary symptoms. These can include painful intercourse, urinary urgency, frequent urination, leakage, burning sensations, recurrent vaginal and urinary tract infections, and vaginal dryness. Collectively, these symptoms are part of the Genitourinary Syndrome of Menopause (GSM). Additionally, many women experience pelvic floor dysfunction, which affects nearly 50% of women by their 50s and can overlap with GSM symptoms.
While systemic hormonal therapy is commonly used to manage menopause symptoms, it may not address the specific needs of those experiencing GSM. The North American Menopause Society recommends the use of vaginal estrogen as an effective treatment for alleviating GSM symptoms and improving quality of life.
Differential Diagnosis:
GSM or Pelvic Floor Dysfunction
Symptoms of pelvic floor dysfunction and Genitourinary Syndrome of Menopause (GSM) can overlap and include:
- Urinary urgency, frequency, burning, nocturia
- Feelings of bladder or pelvic pressure
- Painful sex
- Diminished or absent orgasm
- Difficulty evacuating stool
- Vulvovaginal pain and burning
- Pain with sitting

An experienced healthcare provider, whether a pelvic floor physical and occupational therapists or a medical doctor, can conduct several assessments to diagnose pelvic floor dysfunction, hormonal deficiencies, and pelvic organ prolapse. These evaluations include a vulvovaginal visual examination, a Q-tip test to pinpoint areas of pain, and a digital manual examination.
Without appropriate medical management, all women may eventually experience symptoms of Genitourinary Syndrome of Menopause (GSM). Many are unaware that a pelvic floor physical and occupational therapy evaluation can be highly beneficial for addressing the musculoskeletal issues contributing to their discomfort. Combining pelvic floor physical and occupational therapy with medical treatments can be crucial for improving sexual enjoyment and resolving urinary and bowel problems.
Virtual pelvic floor therapy for menopause—contact us to get started!
FACTS
From: https://www.letstalkmenopause.org/further-reading
- Every day, approximately 6,000 women reach menopause.
- In the United States, around 50 million women are currently navigating menopause.
- About 84% of women experience genital, sexual, and urinary discomfort related to menopause, which often does not resolve without intervention, yet fewer than 25% seek assistance.
- An estimated 80% of OB-GYN residents acknowledge feeling inadequately prepared to address menopause-related issues.
- Genitourinary Syndrome of Menopause (GSM) is clinically identified in 90% of postmenopausal women, yet only one-third report experiencing symptoms in surveys.
- Barriers to treatment include women needing to initiate discussions about their symptoms, a belief that these issues are simply part of aging, and a failure to connect symptoms with menopause.
- Only 13% of healthcare providers routinely inquire about menopause-related symptoms with their patients.
- Even after a diagnosis of GSM, many women remain untreated. This is partly due to healthcare providers’ reluctance to prescribe treatments and patients’ concerns about the safety of topical vaginal therapies, despite evidence showing that GSM significantly affects quality of life.


Hormone deficiency can lead to itching in the labial and vaginal areas. Additionally, other dermatological conditions, such as Lichen Sclerosus and cutaneous yeast infections, should also be considered.
During menopause, individuals are particularly susceptible to frequent vaginal and urinary tract infections due to:
- pH and tissue changes
- incomplete bladder emptying
- pelvic organ prolapse compromising urinary function
Recurrent infections are a major contributor to pelvic floor dysfunction. It’s crucial to address these infections promptly, as ongoing visceral-somatic input from untreated infections can lead to increased pain and further dysfunction even after the infection has been resolved. Without appropriate hormone therapy, infections may persist, leading to severe consequences. Untreated infections can cause unprovoked pain, make sexual activity difficult or impossible, and undiagnosed urinary tract infections (UTIs) may progress to kidney issues and other serious complications.
We recommend consulting with a menopause specialist to effectively monitor, prevent, and treat Genitourinary Syndrome of Menopause (GSM) since these issues are both significant and manageable. It’s important to normalize discussions about GSM; there’s no need for embarrassment. With appropriate care, individuals can lead fulfilling lives. Combining virtual pelvic floor physical and occupational therapy with medical management is essential for optimal results.
Treatment:
How We Can Help You

If you’re experiencing sexual dysfunction, it’s beneficial to consult a pelvic floor physical and occupational therapists online. They can assess whether any issues with your pelvic floor are contributing to your symptoms. During your initial virtual evaluation, the therapist will review your medical history, including previous diagnoses, treatments, and their effectiveness. They understand that many patients feel frustrated by the time they seek help.
The therapist will examine your nerves, muscles, joints, tissues, and movement patterns. After the assessment, they will discuss the findings with you and set both short-term and long-term therapy goals. Typically, physical and occupational therapy sessions occur once or twice a week over a period of approximately 12 weeks. Your therapist will also coordinate with other specialists on your treatment team and provide you with a personalized home exercise program. Our goal is to support your recovery and help you achieve the best possible quality of life.
Get virtual pelvic floor therapy for menopause. Book your online consultation today!

Treatment:
How We Can Help You
If you are having issues with your sexual function, it is in your best interest to get evaluated by a therapist for pelvic floor therapy, so they can establish what part, if any, of your pelvic floor may be contributing to the symptoms you are experiencing. During the course of the examination, the physical and occupational therapists will talk to you about your medical history and symptoms, including what you have been previously diagnosed with, the treatments or therapies you have had, and how effective or ineffective these therapies have been for you. It is significant to mention that we fully comprehend what you’ve been dealing with and that the majority of individuals are angry by the time they make it to see us. The physical and occupational therapists will conduct an evaluation of the patient’s nerves, muscles, joints, tissues, and movement patterns while doing the physical examination. After the examination is finished, your therapist will go over the results of the assessment with you. The physical and occupational therapists will conduct an evaluation to determine the cause of your symptoms and will establish both short-term and long-term therapy goals based on the results of the evaluation. Physical therapy treatments are typically administered between once and twice each week for a period of around 12 weeks. Your physical and occupational therapists will assist you in coordinating your recovery with all the other experts on your treatment team. They will provide you with an exercise regimen to complete at home and the sessions you attend in person. We are here to assist you in getting better and living the best life possible.
Get virtual pelvic floor therapy for menopause. Book your online consultation today!
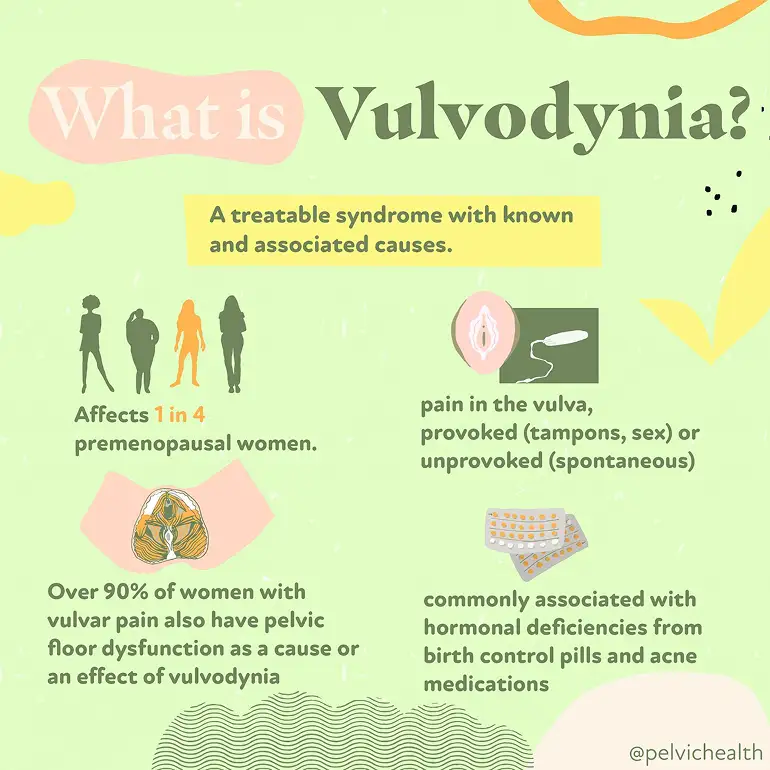
Table of Contents
-
.
-
.
-
.
-
.
-
.
-
.
-
.
-
.
-
.
When Should I See a Pelvic Floor Physical and Occupational Therapists?
-
.
Living with vulvar pain can feel confusing, frightening, and isolating. But despite what you might have been told, vulvodynia is not an unresolvable mystery—it is a symptom with identifiable contributors and effective treatments. Research shows that vulvar pain affects a large number of women over the course of their lives, and more clinicians now recognize it and provide targeted care. By understanding what vulvodynia actually is and how it presents, you can move toward treatment and relief.
As pelvic floor physical and occupational therapists, our team at PHRC works closely with individuals who have spent years searching for answers for their pain, often seeing multiple providers before receiving an accurate diagnosis. Through a combination of expertise, evidence-based care, interdisciplinary management with trusted colleagues, and a deep understanding of the pelvic nervous and musculoskeletal system, we help clients find relief, regain function, and feel like themselves again.
What is Vulvodynia?
The word vulvodynia literally means “pain in the vulva,” which refers to the external female genital area that includes the clitoris, labia, mons pubis, and vaginal opening. It’s best understood as a descriptive term for a symptom rather than a single diagnosis.
So, while vulvodynia sounds like a catch-all label, it actually reflects a variety of underlying and often treatable conditions. Treatment requires identifying the specific contributors—which can be muscular, hormonal, inflammatory, neurological, and psychological—and customizing care to each individual.
What are the Symptoms of Vulvodynia?
Vulvodynia symptoms can vary in type and intensity and can come and go. Some women describe a:
- Constant burning or raw sensation
- Sharp, stabbing, or itching pain
- Pain that is provoked by touch (such as during tampon insertion), sexual activity, or a pelvic exam
- Pain that occurs spontaneously without a known trigger the person can identify
The pain can occur in the labia, clitoris, perineum, and/or vestibule.
What Causes Vulvodynia?
Vulvodynia does not typically come from one single source. Instead, it usually develops from several overlapping factors that interact with one another. Among these, dysfunction of the pelvic floor muscles plays a central role (the pelvic floor muscles support the pelvic organs). Many women with vulvodynia have what’s known as a hypertonic or high-tone pelvic floor. This means the muscles remain overly tight throughout the day, which can compress nerves and blood vessels, reduce circulation, and amplify pain signals. This muscular tension also makes sexual activity, tampon use, or even sitting for long periods more uncomfortable.
Aside from pelvic floor dysfunction, additional contributors can include:
- Hormonal factors, such as reduced estrogen affecting vulvar and vestibular tissue health
- Inflammatory changes in the vulvar or vestibular tissue
- Neurological drivers, including nerve irritation or heightened pain signaling
- Genetic predisposition that increases sensitivity to pain
- Structural issues in the vulvar or vaginal tissues
- Psychosocial influences such as stress, anxiety, or past trauma, which can heighten pelvic muscle tension and pain perception
Because these causes often overlap, vulvodynia is best understood through a biopsychosocial lens. That means a thorough evaluation considers the physical, neurological, hormonal, and emotional factors together. Pelvic floor assessment is a very important part of this evaluation, since muscular overactivity is so common in women with vulvodynia. Once contributors are identified, treatment can begin, often involving a team that includes gynecologists, pelvic floor physical and occupational therapists, and sometimes mental health or pain specialists.
What Role Does Pelvic Floor Dysfunction Play in Vulvodynia?
Pelvic floor dysfunction is one of the most significant contributors to vulvodynia, with research suggesting that anywhere from 20 to 90 percent of people with vulvodynia or vestibulodynia (a form of vulvar pain that affects the tissue around the vaginal opening) also experience pelvic floor dysfunction.

The pelvic floor muscles support the pelvic organs, help control bladder and bowel function, and play an important role in sexual activity. When these muscles are in a constant state of overactivity (called hypertonus or high-tone dysfunction), they can cause pain on their own and amplify pain signals coming from the vulvar tissues.
In women with vulvodynia, the pelvic floor muscles are often found to be:
- Tight and overactive, creating constant pressure in the pelvis
- Tender to the touch, reproducing the same pain felt at the vulva
- Poorly coordinated, making penetration painful and sometimes limiting relaxation even outside of sexual activity
This chronic muscle overuse can compress the blood vessels and nerves, restrict healthy circulation, and keep pain pathways activated. It also explains why symptoms often flare with tampon insertion, penetrative sex, pelvic exams, or even prolonged sitting.
While not every case of vulvodynia involves the pelvic floor, it is much more common to see them together than separately. For this reason, a pelvic floor muscle exam is a very important part of evaluating vulvodynia, and treatment frequently includes pelvic floor physical or occupational therapy to restore normal muscle tone, function, and coordination.
By focusing on the pelvic floor, many women experience meaningful relief—not only of vulvar pain, but also of related issues such as painful intercourse, urinary urgency, or bowel discomfort that can accompany muscle overactivity.
How Is Vulvodynia Diagnosed?
Because vulvodynia is a symptom rather than a single disease, diagnosis begins with ruling out other conditions that might explain the pain. At PHRC, your pelvic floor physical and occupational therapist will start with a detailed health history and a pelvic exam. During the exam, they look for visible changes in the vulvar tissue, signs of infection, or skin conditions that could cause discomfort.
With gentle pressure applied to different areas of the vulva and vestibule, they can map out where your pain occurs and how severe it feels. This helps identify if the pain is localized (such as in the vestibule) or more generalized across the vulva.
Diagnosis often involves a team approach. It is important to know that the majority of general OBGYNs likely did not receive training in medical school about vulvovaginal pain disorders. This surprises many people when vulvodynia symptoms arise, your regular doctor may not be able to diagnose and help you. Medical experts with advanced training and interest in vulvaginal pain disorders can help make the diagnosis. If an expert is not available in your area we recommend the Find a Provider List from the International Study for the Society of Women’s Sexual Health and the International Pelvic Pain Society.
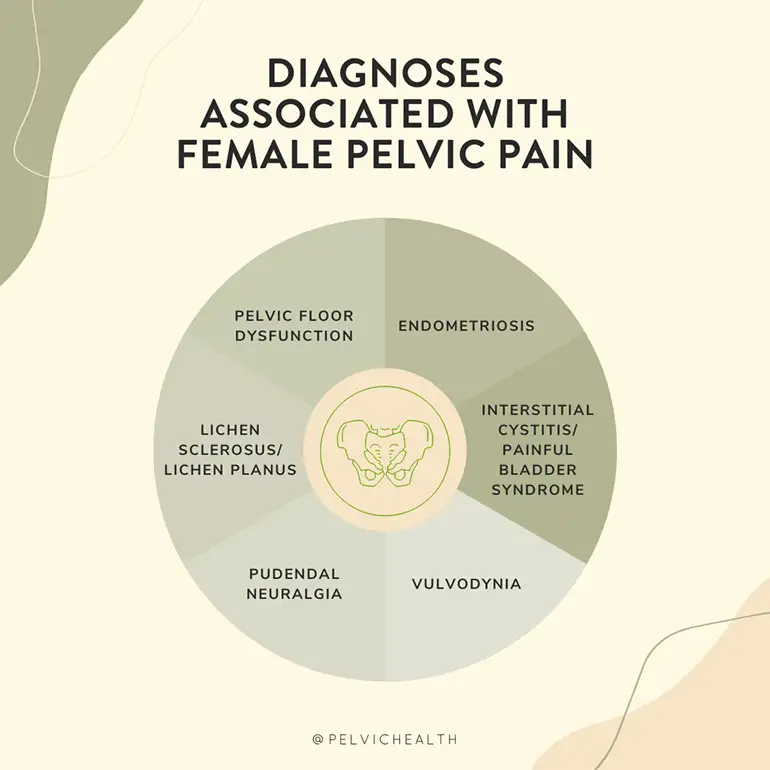
What are the Associated Diagnoses?
In addition to pelvic floor dysfunction causing vulvodynia, it can also be associated with:
- Dyspareunia (painful intercourse), often related to pelvic floor overactivity
- Vaginismus, where pelvic floor muscle contractions make penetration difficult or impossible
- Bladder Diagnoses, such as Interstitial Cystitis
- Bowel Dysfunction, such as constipation
- Other chronic pain conditions, such as irritable bowel syndrome, fibromyalgia, or temporomandibular joint disorder, which reflect a tendency toward central pain sensitization
What is the Treatment for Vulvodynia?
Vulvodynia can sometimes require a combination of treatments. Ultimately, the exact treatments for you will depend on the specific cause of your symptoms and the associated impairments. Below are the most common treatments used by a pelvic floor physical and occupational therapist:
- Manual therapy to release trigger points in pelvic muscles
- Internal and external techniques to ease tightness and improve mobility
- Manual biofeedback to increase awareness and motor control of the pelvic floor muscles
- Training in diaphragmatic breathing to lengthen and relax muscles
- Guided practice in “dropping” the pelvic floor for pain relief
- Gentle stretching positions like child’s pose with coordinated breathing
- Neuromuscular re-education to retrain how pelvic muscles respond to movement
- Exercises that improve blood flow and reduce nerve irritation
- Education on posture and daily habits that can affect pelvic tension
- Home program with relaxation and mobility strategies to support progress
Alongside working with a pelvic floor physical and occupational therapist, some people with vulvodynia find temporary relief from warm sitz baths to soothe irritated tissues and using topical creams or other medications that calm nerve sensitivity.
How Pelvic Floor Physical and Occupational Therapy Helps
Pelvic floor physical and occupational therapy can help with vulvodynia in many ways:
- Relieves burning, stinging, or aching sensations
- Loosens tight pelvic floor muscles
- Improves blood flow and tissue health
- Restores comfortable movement and mobility
- Reduces nerve sensitivity and irritation
- Builds strength and support in the pelvic muscles
- Improves posture and body alignment
- Provides strategies for pain flare management
- Supports sexual function and comfort
What To Expect During a Pelvic Floor Physical and Occupational Therapy Session
At your first visit with PHRC, we take the time to listen to your story. We’ll discuss your symptoms, medical history, past treatments, and how those treatments worked (or didn’t). Many people with vulvodynia come to us after feeling discouraged by multiple appointments and treatments that didn’t help, and we understand how overwhelming that can feel.
During the physical exam, we gently assess your pelvic muscles, connective tissue, nerves, and movement patterns. This hands-on evaluation helps us identify what might be contributing to your pain and discomfort.
After the assessment, we share what we found and explain how these findings connect to vulvodynia. From there, we work with you to create a treatment plan that includes both short-term and long-term goals. Most people benefit from one to two sessions per week for about 12 weeks, along with a home program that supports your progress between visits.
Throughout your care, we also coordinate with your broader medical team to keep your treatment consistent and collaborative. Our goal is to reduce your pain, restore comfort, and help you move forward with more ease in your daily life.
Tips for Living with Vulvodynia
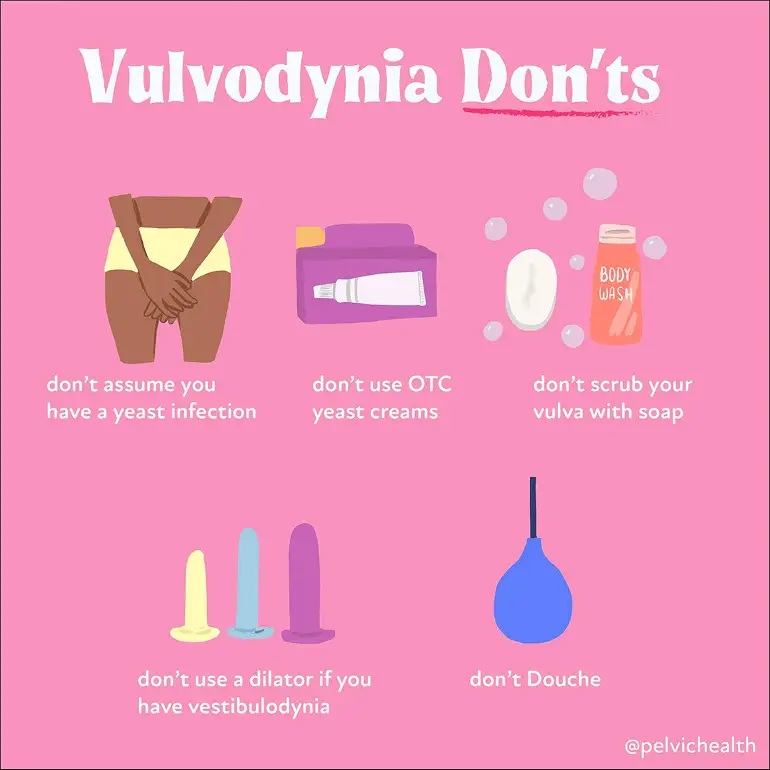
Always Get Tested If You Suspect an Infection
Burning, itching, or irritation can certainly come from infections, but this isn’t always the case. Treating symptoms as though they are an infection without proper testing can delay the right diagnosis. If cultures come back negative, it’s important to look deeper, as many non-infectious conditions (including vulvodynia) can cause similar symptoms.
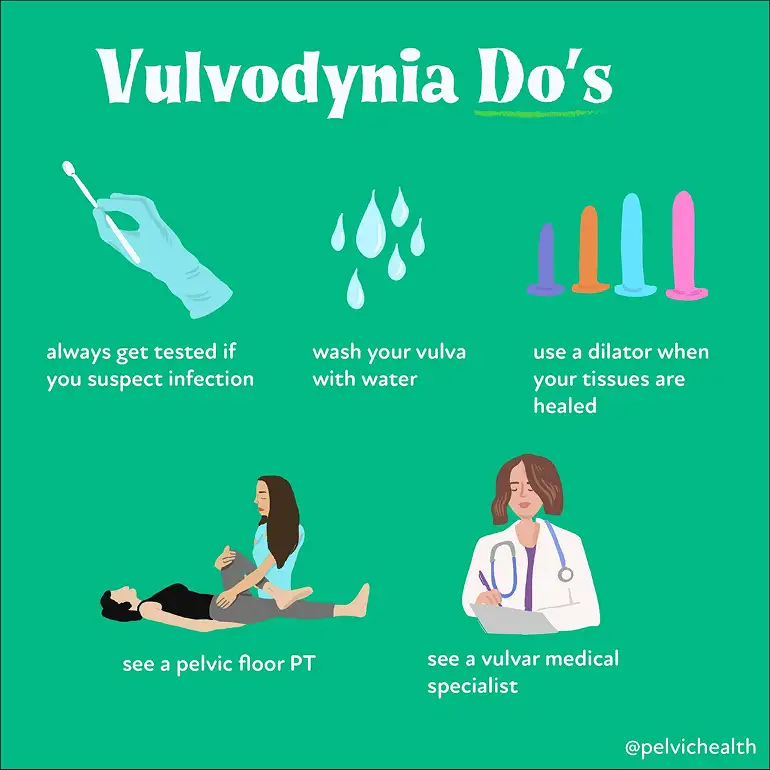
Wash Your Vulva with Water
The vulva does not need soap for good health. Many soaps and body washes contain fragrances, dyes, and other ingredients that can irritate sensitive vulvar tissue. Warm water is enough to keep the area clean.
Use Dilators Only When Your Tissues are Ready
Dilators can be helpful tools for reducing pain with penetration, but only when introduced at the right stage of treatment. Using them too early, or without proper guidance, can increase pain and frustration. A pelvic floor physical and occupational therapist can guide you on when and how to use dilators safely.
See a Pelvic Floor Physical and Occupational Therapist
Pelvic floor dysfunction is a major driver of vulvodynia symptoms. Working with a pelvic floor physical and occupational therapist who has advanced training in pelvic pain can make a real difference.
Get Help Today at PHRC
At PHRC, we’re here to listen, assess, and guide you toward meaningful relief. We take a whole-body approach to care, focusing not just on your painful symptoms but on the underlying patterns that contribute to them.
Our team of pelvic floor physical and occupational therapists brings both clinical expertise and genuine compassion to every session. We work with you to build a plan that fits your life and helps you move forward.
If getting to the clinic is a challenge, we offer telehealth appointments following your first in-person visit, so you can keep making progress no matter where you are.

One Big Beautiful Bill Act: The Impact on Pelvic Health Physical and Occupational Therapy
By Stephanie Prendergast, MPT, PHRC Pasadena
In July 2025, the One Big Beautiful Bill Act (OBBBA) was signed into law, introducing transformative student-loan reform that will shape federal graduate borrowing for decades to come. Among its many sweeping policy changes, one stands out for the rehabilitation community: a recalibration – and dramatic narrowing – of what counts as a “professional degree” for the purpose of federal student loans. The ripple effects for physical and occupational therapists, Medicare beneficiaries, and the broader U.S. health-care system are profound.
For providers working in specialized, high-needs areas such as pelvic health rehabilitation – clinically managing conditions like urinary incontinence, sexual pain disorders, and bowel dysfunction – the implications feel deeply personal. But beyond personal frustration lies a structural reckoning. This law risks destabilizing our clinical pipeline, restricting educational access, and ultimately reducing care availability for the patients who need us most.
The Legislative Change – and who it leaves behind
The OBBBA eliminates Grad PLUS, replacing it with a bifurcated definition of post-baccalaureate borrowing:
- Students enrolled in designated “professional degree programs” may receive up to $50,000 annually, with a $200,000 lifetime cap.
- Students in all other graduate programs – classified under new policy as “non-professional degree programs” – are capped at $20,500 annually, with a $100,000 lifetime borrowing limit, representing an effective reduction of roughly 50% compared to prior borrowing norms.
The list of approved “professional degree programs” remains largely unchanged from legacy policy definitions, emphasizing physician and select medical specialties including: physicians, pharmacists, and attorneys.
Notably excluded from this designation, and therefore reclassified as “non-professional degrees”, are: physical and occupational therapists, nurse practitioners, physician’s assistants, certain mental health professionals, and speech-language and audiology doctorates.
This reclassification was confirmed in recent rulemaking commentary, which explicitly noted that rehabilitation professions and graduate therapy degrees are no longer eligible for the professional borrowing limits afforded to medical degrees.
The real-world cost of a semantic downgrade
Language drives policy. Policy drives financing. And financing drives workforce behavior.
Physical and occupational therapists follow a training pathway that rivals many degree tracks deemed “professional” under the new rule. The process includes:
- Four years of undergraduate education
- Three years of clinical doctorate graduate training, including full-time clinical clerkships
- Passing difficult federal and state licensing boards
- Maintaining licensure with required continuing education hours and mandatory clinical competencies
And for those committed to pelvic health rehabilitation – a specialty serving patients with severe, complex, often disabling symptoms – the financial burden climbs even higher. Post-graduate pelvic-health training programs often cost thousands to tens of thousands of dollars, typically paid out-of-pocket, including advanced fellowships, certifications, and residencies.
Impact on pelvic health patients

The pelvic health patient population is often in dire need. Therapists in this area commonly treat conditions such as:
- Pelvic Floor Dysfunction
- Diagnoses such as Endometriosis, Vulvodynia, Vestibulodynia, Interstitial Cystitis, Chronic Pelvic Pain Syndrome, Pudendal Neuralgia
- Neuroplastic pain syndromes
- Urinary and fecal incontinence
Interdisciplinary pelvic pain requiring both rehab and medical management.
Crucially, evidence consistently shows that medical management alone is rarely sufficient for treating chronic pelvic pain and dysfunction – a fact that underscores the need for interdisciplinary rehabilitation. Pelvic-health therapists do not “replace” medicine – we partner with it, addressing neuromuscular impairments, functional disability, tissue sensitivity, behavioral pain-science education, and return-to-life outcomes that pharmaceuticals alone cannot restore.
If therapist numbers decline, so does the patient’s ability to achieve continence, sexual function, and pain reduction, all of which directly influence psychosocial participation, mobility independence, sleep, emotional health, and societal productivity.
Medicare: coverage vs capacity vs reality
The OBBBA does not directly amend Medicare coverage rules for therapy – but its indirect impact on the coverage landscape may be even more powerful.
Therapy reimbursement under Medicare is governed largely by:
- The Centers for Medicare & Medicaid Services
- Budget-neutrality requirements
- Therapy caps historically imposed and intermittently removed
- Relative Value Unit (RVU) classifications that often undervalue rehabilitative care
Even before OBBBA, rehab providers have weathered perennial reimbursement erosion despite rising overhead costs – supplies, clinic leases, documentation compliance systems, liability insurance, and salary competitiveness.
If clinician supply drops, payors are likely to see PT and OT services as less central – more discretionary, further compromising future payment schedules for therapy, just as we see rising barriers for care access in underserved populations including rural communities, Medicaid beneficiaries, and disabled Medicare recipients.
Already, non-physician graduate providers such as nursing and rehab professions have voiced national opposition, warning that the policy threatens clinician access, patient care access, and educational affordability.
Provider frustration and burnout: a documented crisis
Working in health care is a constant battle. Rehab providers face:
- High student-loan burden
- Salaries that often fail to keep pace with inflation
- Declining reimbursement rates
- High documentation burden for insurance compliance
- Specialty training costs largely out-of-pocket
- Longer patient waitlists with fewer clinicians
- Rising provider burnout across allied health
Meanwhile, private insurance stakeholders continue posting record profits. For example:
- UnitedHealth Group
- Humana Inc.
Insurance profits have rarely correlated with rehab care sustainability – and the result is visible: burned-out clinicians and suffering patients with less access to skilled providers.
National journalism has already warned of clinician outrage and pipeline risk, particularly for professions excluded under the new borrowing rules like nursing and rehabilitation.
When patients pay the price for policy abstraction
If nothing changes, federal policy could fuel cascading harm:
- Fewer students able to afford PT/OT doctorate programs
- Fewer clinicians able to afford pelvic-health specialization
- Longer wait times
- Clinic closures or capacity reductions
- Fewer interdisciplinary partners for pelvic pain care
- Lower reimbursement justification due to workforce scarcity
- Patients left untreated – or under-treated
This means that patients suffering pelvic pain or dysfunction might wait months to be evaluated, lose access to conservative care options entirely, or be returned to a solely medical path that is statistically less sufficient for functional restoration.
The call to action
This is a moment for advocacy – not passive acceptance.
Professional associations including the American allied-health coalition have already mobilized opposition, warning that programs like DPT and OTD are essential, intensive, and must be recognized as professional-level training tracks to preserve our workforce pipeline and patient access to care.
If the rulemaking definition can be updated to reflect modern educational rigor and clinical necessity, the damage could still be mitigated. But if nothing changes, we risk losing the next generation of pelvic-health therapists – and our patients will suffer most.

______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical therapists via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
By Stephanie Prendergast, MPT, PHRC Pasadena
Many people think of Restless Leg Syndrome (RLS) as a sleep-related leg problem ; the irresistible need to move, the creeping sensations, the nights spent pacing instead of resting. But growing research and clinical observation suggest something much broader: RLS may be part of a whole-body sensory and motor dysregulation, with ties to bladder symptoms and pelvic floor dysfunction, including a number of pelvic pain syndromes.
At the Pelvic Health and Rehabilitation Center (PHRC), we’ve seen this overlap firsthand. Patients with persistent pelvic tension or ‘tightness’, urinary urgency and/or frequency, irritative bladder symptoms, or genital discomfort sometimes describe “restless” sensations not just in their legs, but deep in their pelvic structures. Understanding these links helps us design more comprehensive treatment plans that address both the pelvic floor and the nervous system that governs it.
Understanding Restless Leg Syndrome in Context
As outlined in our previous post, RLS is a neurological condition characterized by an urge to move the legs, especially at night or during rest. It’s thought to arise from dopaminergic dysregulation and iron deficiency in the brain, both of which disrupt smooth motor control and sensory processing.
Beyond the legs, the condition reflects a sensory hypersensitivity ; the nervous system becomes overly reactive to otherwise normal sensations. This helps explain why some individuals also experience “restless” or uncomfortable sensations in other regions, including the pelvic and genital area.
Restless Genital Syndrome: A Clue from the Pelvis
A condition called Restless Genital Syndrome (RGS), first described in the early 2000s, presents with sensations of tingling, pressure, or internal agitation in the genital or pelvic region. Importantly, these sensations are not linked to sexual arousal and often worsen at rest, just like RLS.
Neurophysiological studies have shown that some people with RGS also meet criteria for RLS, and both conditions often respond to dopaminergic medications (like pramipexole). This overlap suggests they share a common mechanism ; likely involving the lumbosacral nerves that control both the legs and the pelvic floor.
At PHRC, we think of RGS as part of a continuum of sensory-motor dysregulation. The same central nervous system patterns that drive restless legs ; dopamine imbalance, sensory hyperexcitability, and altered movement feedback ; can easily extend into the pelvic region.
Shared Pathways: The Neurology of RLS and the Pelvic Floor
The pelvic floor is more than a group of muscles; it’s a hub of sensory and motor information, richly connected through the sacral spinal cord and the pudendal nerve. These nerves share close connections with the pathways implicated in RLS.
Here’s how the two systems intersect:
- Shared nerve roots: The lower spinal cord (L2–S3) sends fibers to both the legs and pelvic organs. When these circuits become dysregulated, sensory symptoms may appear in either or both regions.
- Autonomic involvement: RLS is linked to changes in autonomic nervous system activity (fight-or-flight vs. rest-and-digest). Pelvic floor tone is also heavily influenced by autonomic balance ; many people with chronic stress or poor sleep develop hypertonic pelvic floor muscles.
- Neuroinflammation and iron metabolism: Iron deficiency, microglial activation, and dopamine dysregulation seen in RLS may also affect pelvic nerves, influencing pain perception and muscle tone.
- Movement and muscle co-contraction: Just as RLS causes involuntary leg movements, some people experience unconscious pelvic floor tightening during episodes of restlessness or nocturnal movement.
In other words, the restlessness of RLS may extend into the pelvis, resulting in pelvic floor overactivity, urinary urgency, or genital discomfort.
Bladder and Bowel Clues
Several studies have explored the connection between RLS and overactive bladder (OAB). Patients with RLS often report more urinary urgency, frequency, and nocturia (waking to urinate at night). One hypothesis is that both RLS and OAB stem from hyper-responsive sensory circuits in the spinal cord and brainstem.
Similarly, chronic constipation ; common in both pelvic floor dysfunction and RLS ; can worsen sensory feedback loops, leading to further pelvic tension. At PHRC, we see how unaddressed bowel dysfunction perpetuates pelvic and lower limb discomfort.
These observations reinforce the need to look beyond single symptoms. A patient’s nighttime restlessness, urinary urgency, or pelvic pain may all share a nervous-system origin.
The Female Connection
RLS is twice as common in those assigned female at birth, particularly during pregnancy and menopause ; life stages characterized by hormonal shifts that influence both the nervous system and pelvic tissues. Estrogen and progesterone fluctuations can alter dopamine sensitivity, while pregnancy increases venous congestion and iron demands. These same changes can trigger or worsen pelvic floor dysfunction, pelvic pain, or bladder symptoms.
Recognizing these overlapping hormonal and neurovascular influences is critical for accurate diagnosis and individualized care.
How Pelvic Floor Physical and Occupational Therapy Can Help
Even though RLS is a neurological condition, pelvic floor physical and occupational therapy can play a valuable role, especially when pelvic symptoms coexist. Here’s how:
- Muscle down-training and relaxation: Manual therapy, biofeedback, and breathing techniques help calm hypertonic muscles that may tighten reflexively during RLS episodes.
- Nerve mobilization: Gentle neural gliding and positional release techniques support the pudendal and sciatic nerves, improving blood flow and decreasing neural tension.
- Circulatory enhancement: Movement, stretching, and soft tissue work improve lower-body and pelvic circulation, which may reduce discomfort from venous congestion.
- Autonomic regulation: Incorporating mindfulness, diaphragmatic breathing, and body-scan exercises helps reduce sympathetic overactivity ; the same system that amplifies both pelvic tension and RLS restlessness.
- Interdisciplinary care: Collaboration with physicians is essential to address systemic contributors such as iron deficiency, sleep deprivation, or dopaminergic imbalance.
When treatment combines neurologic management and pelvic rehabilitation, patients often notice better sleep, less pelvic tension, and improved quality of life.
Practical Tips for Those With Restless Leg Syndrome and Pelvic Floor Dysfunction
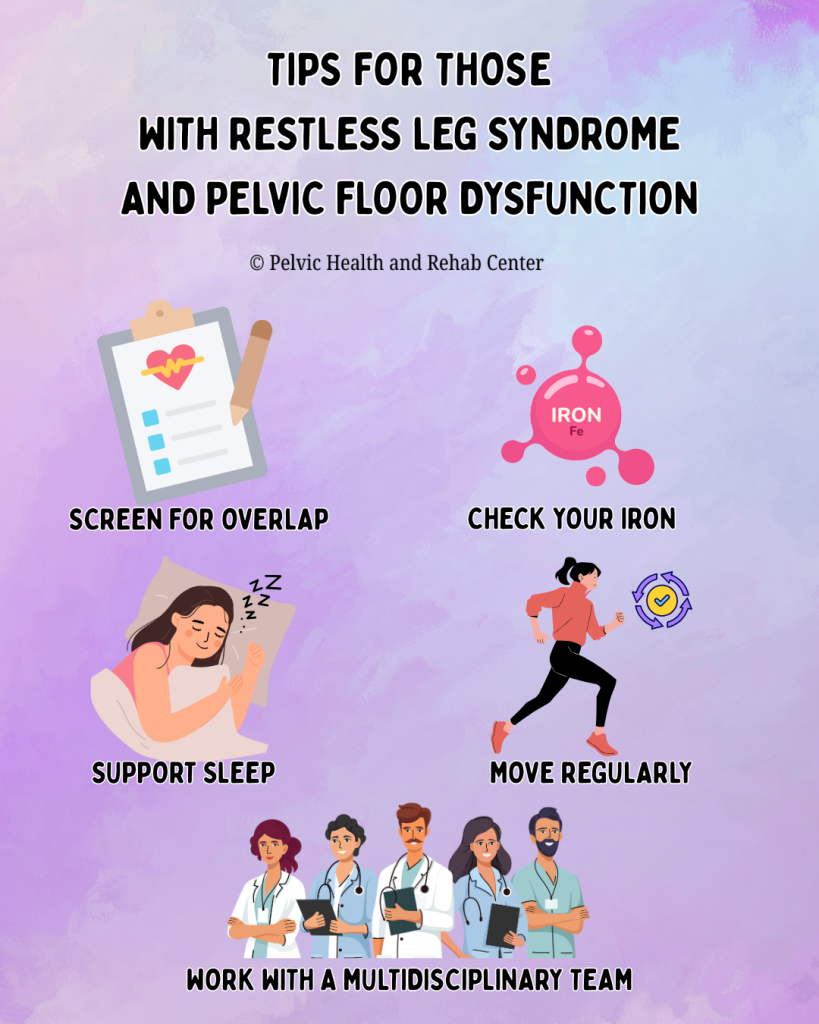
Screen for overlap: If you have pelvic pain or urinary urgency plus nighttime leg restlessness, tell your provider. Both may stem from one nervous-system imbalance.
Check your iron: Ferritin levels below 75 µg/L are linked with RLS; optimizing iron can help both leg and pelvic symptoms.
Move regularly: Gentle evening stretches, walking, or yoga reduce both leg and pelvic tightness.
Support sleep: Consistent bedtime routines, magnesium intake (if appropriate), and stress reduction lower symptom intensity.
Work with a multidisciplinary team: A pelvic health physical therapist, primary care physician, and possibly a neurologist can coordinate a plan that addresses all levels ; muscular, vascular, and neural.
The Takeaway
Restless Leg Syndrome is more than a “leg problem.” It’s a systemic sensory-motor dysregulation that can influence the pelvic floor, bladder, and even sexual function. For some, the pelvis becomes part of the “restlessness loop” ; muscles tighten, nerves fire excessively, and the nervous system can’t find calm.
The good news: once recognized, these connections can be treated. Through integrated care ; neurologic, musculoskeletal, and behavioral ; patients can regain rest, comfort, and control over both their legs and their pelvic health.
At PHRC, we treat the body as an interconnected system. Whether your symptoms start in the legs, pelvis, or both, our goal is to restore balance, reduce tension, and help you feel at home in your body again.
References
Malykhina, A. P. (2007). Neural mechanisms of pelvic organ cross‑sensitization. Neuroscience, 149(3), 660–672. https://pubmed.ncbi.nlm.nih.gov/17920206/
Malykhina, A. P., Sengupta, J. N., et al. (2005). Mechanisms of pelvic organ cross-talk: Impact of colorectal distention on bladder afferent nerve activity. American Journal of Physiology – Regulatory, Integrative and Comparative Physiology, 288(3), R555–R564. https://pubmed.ncbi.nlm.nih.gov/23542407/
Panicker, J. N., Marcelissen, T., von Gontard, A., Vrijens, D., Abrams, P., & Wyndaele, M. (2018). Bladder-bowel interactions: Do we understand pelvic organ cross‑sensitization? International Consultation on Incontinence Research Society. https://pubmed.ncbi.nlm.nih.gov/31821639/
Quaghebeur, J., et al. (2024). Integral theory and pathogenesis of LUTS and chronic pelvic pain. Pelviperineology, 43(1), 30‑39. https://pelviperineology.org/pdf/07d42497-fb2b-47e0-be2f-8805fa940376/articles/PPj.2024.43.01.2023-11-3/Pelviperineology-43-30-En.pdf
Ustinova, E. E., Fraser, M. O., & Pezzone, M. A. (2010). Cross-talk and sensitization of bladder afferent nerves. Neurourology and Urodynamics, 29(1), 77–81. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2805190/
Vlasie, A., Trifu, S. C., Lupuleac, C., & Cristea, M. B. (2021). Restless legs syndrome: An overview of pathophysiology, comorbidities and therapeutic approaches. Experimental and Therapeutic Medicine, 22(6), 1355. https://www.spandidos-publications.com/10.3892/etm.2021.11108
Moral, C., Aydın, M., Yılmaz, A., İrkılata, L., Bitkin, A., & Kırdağ, M. K. (2025). The relationship between restless legs syndrome and overactive bladder: A cross‑sectional, controlled study. International Journal of Urology. https://pubmed.ncbi.nlm.nih.gov/40045817/
American Academy of Sleep Medicine. (2024). Treatment of restless legs syndrome and periodic limb movement disorder: Clinical practice guideline. https://aasm.org/wp-content/uploads/2024/03/Treatment-of-RLS-and-PLMD-CPG.pdf
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical therapists via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!