
Menopause is more than just hot flushes, night sweats and mood changes! Even though 50% of the population goes through menopause the majority of people and healthcare providers are under-informed about menopause and safe and effective treatments. Too many people are suffering unnecessarily. Perimenopause, the precursor to menopause begins in the 40’s for most people and most women will be in menopause by their early 50’s. Beyond the systemic symptoms of menopause people will start to experience more subtle genitourinary symptoms that will continue to worsen over time if untreated. Painful sex, urinary urgency, frequency, leaking and burning, recurrent vaginal and urinary tract infections and vaginal dryness are symptoms of the Genitourinary Syndrome of Menopause (GSM). The symptoms of GSM are also symptoms of pelvic floor dysfunction, which almost 50% of women suffer by the time they are in their 50s.
Systemic menopause symptoms are often treated with systemic hormonal therapy. This may not be sufficient for people developing GSM symptoms. The North American Menopause Society recommends vaginal estrogen for women in menopause to help counter GSM symptoms.
Menopause is more than just hot flushes, night sweats and mood changes! Even though 50% of the population goes through menopause the majority of people and healthcare providers are under-informed about menopause and safe and effective treatments. Too many people are suffering unnecessarily. Perimenopause, the precursor to menopause begins in the 40’s for most people and most women will be in menopause by their early 50’s. Beyond the systemic symptoms of menopause people will start to experience more subtle genitourinary symptoms that will continue to worsen over time if untreated. Painful sex, urinary urgency, frequency, leaking and burning, recurrent vaginal and urinary tract infections and vaginal dryness are symptoms of the Genitourinary Syndrome of Menopause (GSM). The symptoms of GSM are also symptoms of pelvic floor dysfunction, which almost 50% of women suffer by the time they are in their 50s.
Systemic menopause symptoms are often treated with systemic hormonal therapy. This may not be sufficient for people developing GSM symptoms. The North American Menopause Society recommends vaginal estrogen for women in menopause to help counter GSM symptoms.
Differential Diagnosis:
GSM or Pelvic Floor Dysfunction
Symptoms of pelvic floor dysfunction and GSM include:
- Urinary urgency, frequency, burning, nocturia
- Feelings of bladder or pelvic pressure
- Painful sex
- Diminished or absent orgasm
- Difficulty evacuating stool
- Vulvovaginal pain and burning
- Pain with sitting

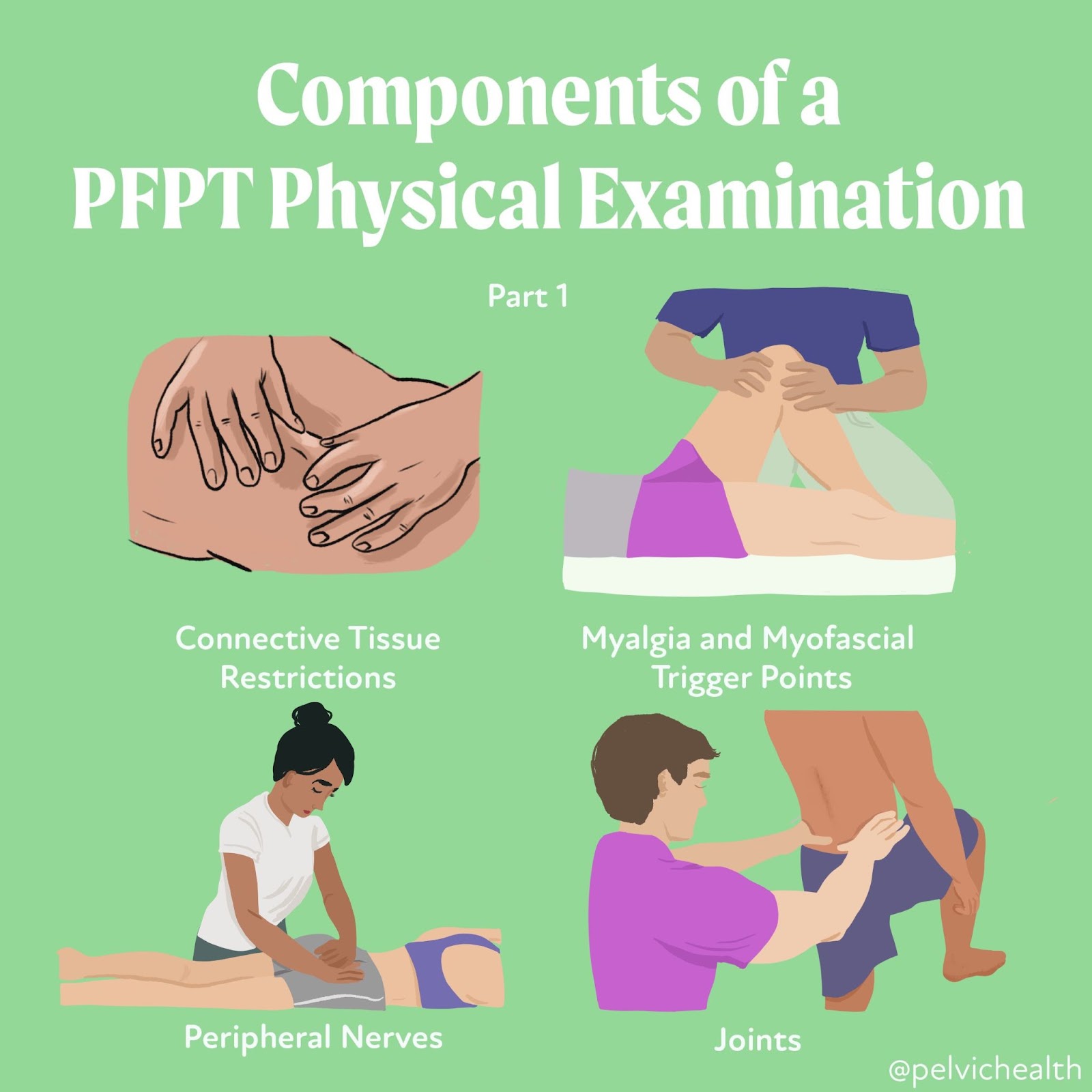
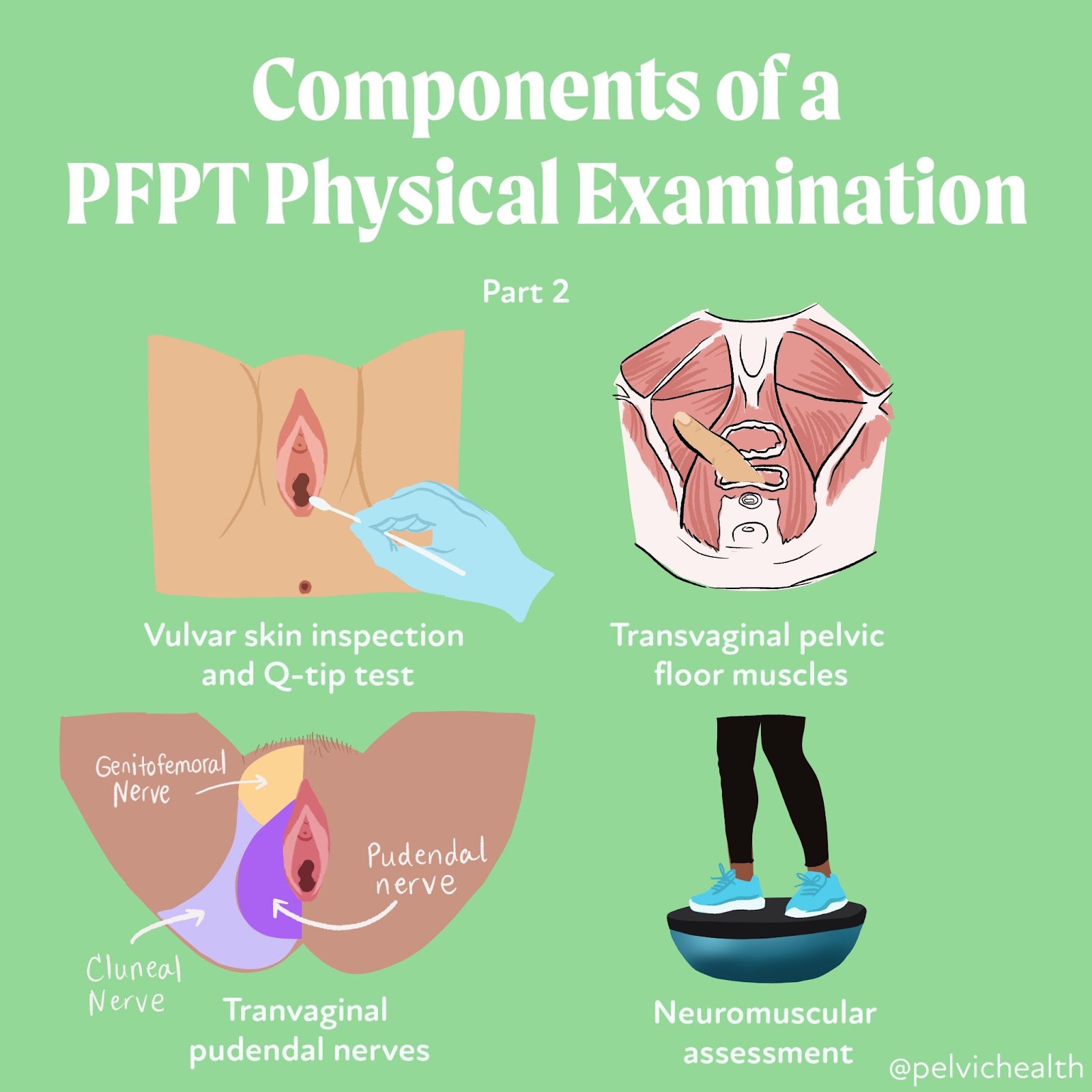
An informed healthcare provider – whether a pelvic floor physical and occupational therapists or medical doctor – can do a vulvovaginal visual examination, a q-tip test to establish pain areas, and a digital manual examination to identify pelvic floor dysfunction, hormonal deficiencies, and pelvic organ prolapse. All women will experience GSM if enough time passes without appropriate medical management. The majority of people do not realize that menopausal women can benefit from a pelvic floor physical and occupational therapy examination to address the musculoskeletal factors that are also making them uncomfortable. The combination of pelvic floor physical and occupational therapy and medical management is key to help restore pleasurable sex and eliminate urinary and bowel concerns!
FACTS
From: https://www.letstalkmenopause.org/further-reading
- 6000 women enter menopause everyday
- 50 million women are currently menopausal in the US
- 84% of women struggle with genital, sexual and urinary discomfort that will not resolve on its own, and less than 25% seek help
- 80% of OBGYN residents admit to being ill-prepared to discuss menopause
- GSM is clinically detected in 90% of postmenopausal women, only ⅓ report symptoms when surveyed.
- Barriers to treatment: women often have to initiate the conversation, believe that the symptoms are just part of aging, women fail to link their symptoms with menopause.
- Only 13% of providers asked their patients about menopause symptoms.
- Even after diagnosis, the majority of women with GSM go untreated despite studies demonstrating a negative impact on quality of life. Hesitation to prescribe treatment by providers as well as patient-perceived concerns over safety profiles limit the use of topical vaginal therapies.


Hormone insufficiency can result in interlabial and vaginal itching. Other dermatologic issues such as Lichen Sclerosus and cutaneous yeast infections are just two of the many factors to also be considered.
Unfortunately people are vulnerable to recurrent vaginal and urinary tract infections in menopause due to:
- pH and tissue changes
- incomplete bladder emptying
- pelvic organ prolapse compromising urinary function
Recurrent infections are a leading cause of pelvic floor dysfunction! They must be stopped or the noxious visceral-somatic input can cause further pain and dysfunction after the infection is cleared. Furthermore, if the infections are left untreated without hormone therapy infections continue to occur and the consequences can be severe. Women can develop unprovoked pain, sex may be impossible, and undetected UTIs can lead to kidney problems and more sinister issues.
We encourage people to work with a menopause expert to monitor, prevent, and treat these issues as they are serious and treatable! We need to normalize the conversation about what happens during GSM, it is nothing to be embarrassed about and with the right care vulva owners can live their best lives! Pelvic floor physical and occupational therapy and medical management go hand in hand.
Treatment:
How We Can Help You

If you are having issues with your sexual function, it is in your best interest to get evaluated by a therapist for pelvic floor therapy, so they can establish what part, if any, of your pelvic floor may be contributing to the symptoms you are experiencing. During the course of the examination, the physical and occupational therapists will talk to you about your medical history and symptoms, including what you have been previously diagnosed with, the treatments or therapies you have had, and how effective or ineffective these therapies have been for you. It is significant to mention that we fully comprehend what you’ve been dealing with and that the majority of individuals are angry by the time they make it to see us. The physical and occupational therapists will conduct an evaluation of the patient’s nerves, muscles, joints, tissues, and movement patterns while doing the physical examination. After the examination is finished, your therapist will go over the results of the assessment with you. The physical and occupational therapists will conduct an evaluation to determine the cause of your symptoms and will establish both short-term and long-term therapy goals based on the results of the evaluation. Physical therapy treatments are typically administered between once and twice each week for a period of around 12 weeks. Your physical and occupational therapists will assist you in coordinating your recovery with all the other experts on your treatment team. They will provide you with an exercise regimen to complete at home and the sessions you attend in person. We are here to assist you in getting better and living the best life possible.
For more information about IC/PBS please check out our IC/PBS Resource List.

Treatment:
How We Can Help You
If you are having issues with your sexual function, it is in your best interest to get evaluated by a therapist for pelvic floor therapy, so they can establish what part, if any, of your pelvic floor may be contributing to the symptoms you are experiencing. During the course of the examination, the physical and occupational therapists will talk to you about your medical history and symptoms, including what you have been previously diagnosed with, the treatments or therapies you have had, and how effective or ineffective these therapies have been for you. It is significant to mention that we fully comprehend what you’ve been dealing with and that the majority of individuals are angry by the time they make it to see us. The physical and occupational therapists will conduct an evaluation of the patient’s nerves, muscles, joints, tissues, and movement patterns while doing the physical examination. After the examination is finished, your therapist will go over the results of the assessment with you. The physical and occupational therapists will conduct an evaluation to determine the cause of your symptoms and will establish both short-term and long-term therapy goals based on the results of the evaluation. Physical therapy treatments are typically administered between once and twice each week for a period of around 12 weeks. Your physical and occupational therapists will assist you in coordinating your recovery with all the other experts on your treatment team. They will provide you with an exercise regimen to complete at home and the sessions you attend in person. We are here to assist you in getting better and living the best life possible.
For more information about IC/PBS please check out our IC/PBS Resource List.



By Jandra Mueller, DPT, MS, PHRC Encinitas
Here at PHRC we regularly discover all sorts of new and cool products that are available for people’s pelvic health needs. I am amazed at some of the products available and that are being developed and am so thankful there are people that are creating these products because they are SOOO helpful! This is an updated version of one of our previous blogs, since there have been some new developments in the last few years and we wanted to share them with you!
Pelvic health physical and occupational therapistss treat a multitude of conditions that can include, but are not limited to, urinary dysfunction, sexual dysfunction, bowel issues (aka pooping), as well as pain in the pelvic region. Pelvic floor dysfunction is not a gender-specific disorder and can affect all people at different phases of their lives.
This week, we wanted to highlight some of our continued go-tos that can help people recover from pelvic pain, specifically painful sex, and introduce some new products that have been developed. There are a variety of pelvic floor disorders that affect daily life; we hope this list helps you receive the best care possible while alleviating any discomfort being experienced. If you see a product on this list that interests you, it may be a good idea to discuss it with your physical and occupational therapists and how it can be implemented into your treatment plan.
Let’s talk about sex baby… and many of the products, tools, and resources available.
Dilators aka “trainers”
Here at PHRC we have quite a few that we are a fan of! Dilators are used to increase tolerance of both vaginal and anal sex for all people, straight, bisexual, transexual, pansexual… literally everyone! There are differences in materials, colors, styles, and pricing so finding the right fit for you is important. Dilators are a great tool to pair up with a regimen of pelvic floor physical and occupational therapy.
 Milli vaginal trainer
Milli vaginal trainer
 Milli vaginal trainer
Milli vaginal trainer This dilator is unique, it is the only expandable dilator yet. This means that you don’t have to insert a series of dilators each time which may eliminate irritation if you have pain with initial insertion. It expands inside of you and you can measure specifically the dilation. Recovering from painful sex can take time, we love that this device helps people objectively measure progress with the digitized face depicting the size it has expanded to. It is made of a soft silicone and it does have a vibrating feature. It comes in its own charging case so it is easier to travel with as well.
 Soul Source Silicone Dilators
Soul Source Silicone Dilators
 Soul Source Silicone Dilators
Soul Source Silicone Dilators
With the release of their new silicone finish, these dilators come in a vast variety of sizes and have different sets to match your needs. They are also made locally in CA! They are a bit on the pricier side, but they are definitely a quality product!
 GRS – Dilator set by Soul Source
GRS – Dilator set by Soul Source
 GRS – Dilator set by Soul Source
GRS – Dilator set by Soul Source
Soul source has made these specifically for those undergoing gender reassignment surgery in conjunction with a surgeon that performs this surgery. These dilators are made of rigid polyurethane, and can be chilled in order to use for post-surgical swelling in addition to using them for general dilation post-surgery.
New Flora Dilator Sets |
She-ology Wearable Dilators |
Intimate Rose Dilator Set |
||
 With a nice smooth silicone finish, these dilators are slightly different in length and size, and are one of the more affordable sets on the market. With a nice smooth silicone finish, these dilators are slightly different in length and size, and are one of the more affordable sets on the market. |

These silicone dilators are like no other. This is the first set of wearable dilators for those that want to try a different position or move around. They also come in a larger, more advanced set.
|

Similar to soul source, these offer soft silicone (maybe even a little softer) and a variety of sizes and sets, and a bit cheaper as well! Silicone in general is nice because it often feels more like human skin instead of hard plastic. |

 Clone-A-Willy
Clone-A-Willy
 Clone-A-Willy
Clone-A-Willy
Yes, you heard it correctly, a cloning kit that allows you to clone your partner! This is for patients working specifically towards a goal of pain-free intercourse with their partner who may have anxiety/have a hard time communicating their needs during intercourse with their partners. Also comes in a variety of colors, and it even glows in the dark!
New Flora Pelvic Wand

Intimate Rose Pelvic Wand

Many patients ask us, “so how can I do this on my own?” Well, the pelvic wands offer just that. With the S-shape meant to help with your ergonomics of gripping, this slides right in and allows you to access your pelvic floor muscles. With the tapered end, it’s great for trigger point release. They also offer a wand with a vibrating feature as well. There are now a couple on the market, both offering vibrating options, though each have a slightly different shape.

Ohnut!
Made for the people, by the people. This device made by The Pelvic People, was developed for those that have pain with deep penetration. They are very soft, stackable rings that go on the male partner to create essentially a buffer so that penetration does not go so deep, yet both partners still feel pleasurable. They now offer an additional vibrating ring to enhance pleasure!
 The Kiwi
The Kiwi

Featuring the newest product from The Pelvic People, this device is a two-for-one. With the ability to help you tackle pelvic pain and progress towards pleasure, this is one of the best devices on the market right now! Offering a dual control vibration and multiple options for use, we give it 5 stars!
Personal Lubricants
To begin, there are a ton of personal moisturizers aka lubricants out there that are better used for anal vs. vaginal use. These depend on both the pH of the product as well as the osmolality. And there are things to consider like water-based or oil-based. SO. MANY. OPTIONS!
Lube + Sperm:
- The best conditions for sperm survival and motility is pH 7.2-8.5 and osmolality 270-360 mOsm/kg.
- Brands: Pre-Seed, Yes Baby
Vaginal and Rectal pH
- Vaginal: 3.8 – 4.5
- Rectal: 7.0
Osmolality
- The World Health Organization (WHO) recommends osmolalities of less than 380 mOsm/kg
- Silicone-, Plant, and Oil-based lube are also less likely to irritate, but their osmolality cannot be measured.
For a more in depth review about why lube selection is important, one of our senior physical and occupational therapistss, Melinda Fontaine (Walnut Creek, CA), wrote a blog that you can read here.
What we use in the clinic:



Typically we use slippery stuff for our transvaginal work and surgilube for transrectal work. Releveum is now classified as a moisturizer because it can be used for longer than 60 minutes, while lubes are short-term and do not last longer than 60 minutes. Releveum is an aloe vera based lube/moisturizer. It contains 4% lidocaine that can be used to help soothe or numb burning tissue, like for those that have pain with initial penetration and suffer from Vestibulodynia, and can help in the short-term for improving that pain!
Moisturizers and other care products for “down there”
There are some other moisturizers that can be helpful for irritated tissue, especially if you don’t want to, or cannot use hormones for any reason. There are two that we often recommend for women that have pain with initial penetration from irritated or inflamed tissue at the entrance of the vagina and the vestibule. I often recommend them for my mama’s that are pregnant or postpartum and CANNOT use any hormones (even local ones) because it is contraindicated in pregnancy and postpartum. This is also true for those women who are concerned about, or would feel more comfortable not using hormones because they have had certain types of cancer.
Vital V V-Magic

![]()
These are both used to soothe the tissues, but have slightly different ingredients. Vital V has vitex, which is chaste berry extract while Vmagic has some ingredients that are more antimicrobial. We use them both and it may just be a personal preference of which may work for you!
 Kindra
Kindra
 Kindra
Kindra
The Daily Vaginal Lotion features a blend of ultra-hydrating extracts to support skin-moisture barrier healing for vulvar and vaginal dryness. Whereas the V Relief Serum features a biomimetic peptide clinically studied to reduce skin sensitivity and reactivity, including stinging, burning, and itching.
Education
If you have ever been a patient here at PHRC, visited our office, or seen our videos on social media, you know how valuable education is to us!

When Sex Hurts

Pelvic Pain Explained

PHRC’s First E-Book!
Our favorite books to recommend are “When Sex Hurts” which has been updated with SO much new information about the causes of painful sex and what you can do about it, authored by some of the top pelvic health specialists in the world. “Pelvic Pain Explained” which was co-authored by PHRC’s co-founders Stephanie Prendergast (Pasadena, CA) and Elizabeth Akincilar (Merrimack, NH) and PHRC’s very first e-book “Vulvodynia, Vaginismus, & Vestibulodynia: Your guide to diagnosis and treatment” by Stephanie Prendergast, Elizabeth Akincilar, and Jandra Mueller. You can find this book for $10 on our website. We’ve compiled so many of the resources we’ve collected over the years into a fun, digestible book for patients to get the help they need
Your toolbox does not need to just be manual therapy techniques! If you have feedback about these products we’d also love to hear so feel free to comment below and share some of your favorites! We love to hear back from patients and healthcare providers about the types of products they use as treatment options.
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Did you know we opened our 11th location in Columbus, OH? Now scheduling new patients- call (510) 922-9836 to book!
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
By Stephanie Prendergast, MPT, Cofounder, PHRC Pasadena
Urinary leaking during sneezing and coughing is common. Constipation affects millions of people. Irritative bladder symptoms plague women at multiple points in their life for a number of reasons, and bother men too. If one stops to think about orthopedic surgeries for broken ankles and shoulder dysfunction, why isn’t pelvic floor physical and occupational therapy part of the standard of care after all pelvic surgeries?
If you fall into any of the categories listed above you should consider an evaluation with a pelvic floor physical and occupational therapists. When people find us on their own their first question is often “why didn’t my doctor tell me?.” The fact is almost all medical schools lack information on various pelvic pain and pelvic floor disorders and therefore most physicians do not know that pelvic floor physical and occupational therapy exists and can help their suffering patients!
Let’s explain these six reasons that no one thinks to call a PT about:
Urinary leaking
Leaking urine is a symptom. Millions of people leak, and therefore this treatable symptom gets chalked up to part of the aging process or because you just had a baby. The reality is leaking is a sign of pelvic floor dysfunction and it should be addressed
Constipation
Constipation also plagues millions of people. In order for humans to evacuate stool the pelvic floor muscles have to autonomically and voluntarily relax. If the muscles are not functioning properly constipation can occur.
Bladder irritability
Irritative bladder symptoms can be miserable. Did you know pelvic floor dysfunction can mimic the symptoms of urinary tract infections? One should always undergo cultures to rule out infection. If the cultures are negative, consider an evaluation with a pelvic floor physical and occupational therapists.
Postpartum
All postpartum women should see a physical and occupational therapists. Pregnancy, labor and delivery are exceptional physiological situations and women need to rehabilitate afterwards.
Gender affirming surgery
Gender affirming surgeries essentially reorganize the pelvis. We are here to help people recover and live their best life!
Pelvic Surgery
Pelvic surgeries such as prostatectomy, pelvic organ prolapse repair, and hysterectomy are major surgeries that influence how your pelvic floor functions. Pelvic physical and occupational therapy should be offered prior to surgery to help with recovery and after surgery for rehabilitation.
While all of these scenarios are common, they are not normal and a sign of pelvic floor dysfunction. A good pelvic evaluation will help you learn what your individual impairments are and how to help.
Common reasons for these symptoms and pelvic floor dysfunction exist.
In general, most symptomatic people fall into one or a combination of these categories:
- Tight and painful pelvic floor and girdle muscles.
- Weak pelvic floor and girdle muscles.
- Tight and weak pelvic floor muscles.
- Coordination issues of the pelvic floor and girdle muscles.
- Presence of a diastasis recti.
- Nerve or muscle involvement after surgery or childbirth.
The pelvic floor muscles are an integral part of our core, playing crucial roles in urinary, bowel, and sexual function, as well as contributing to our overall comfort. Seemingly minor symptoms, such as leaking when sneezing, indicate that these muscles are not functioning optimally. It is important to seek evaluation and treatment early to prevent the development of more significant and disruptive symptoms.
While general categories of impairment exist, people with the same symptoms often have different underlying causes. This is why we do not use protocols, a one-size-fits-all approach is more like one-size-fits none. We pride ourselves on helping our patients best understand their bodies and help them restore their pelvic health!
How Do We Do Pelvic Floor Physical and Occupational Therapy?
At PHRC we focus our in-person visits on things our patients cannot do for themselves. This may include manual therapy such as myofascial release and connective tissue manipulation, joint manipulation and neuromuscular re-education. We also provide impairment-specific home exercises to lengthen, strengthen, or help to improve neuromuscular control. We establish short term goals that are typically expected to be achieved in six to eight visits. We also establish long term goals which are tied to someone’s desired functional outcome, such as not leaking, having easy bowel movements, and urinating no more than six to eight times in a 24 hour period with distress or urgency. People should not have to think about their bladders!
People often ask if they have to do their exercises and home program forever. The answer is it depends, sometimes yes and sometimes no.
Have questions? So do many other people. Please see our FAQ list below and message us with your comments and questions!
Frequently Asked Questions
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor therapy?
Pelvic floor therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapists need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The pelvic floor physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for three months to a year.
______________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Did you know we opened our 11th location in Columbus, OH? Now scheduling new patients- call (510) 922-9836 to book!
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
By Cambria Oetken, PHRC Westlake Village
June is Men’s Health month, and men suffer from pelvic pain too. Research shows that up to 16% of men suffer from Chronic Pelvic Pain Syndrome (CPPS) at some point in their life. However, we suspect this number is lower than the actual prevalence because it is so commonly misdiagnosed as a bacterial infection aka prostatitis. In today’s post we are going to share an all-too-common problem men face and the pelvic floor physical and occupational therapy solutions. Keep reading through the end to hear what Josh had to say in his own words.
Background
Josh is a 27-year-old male who came to PHRC with a 3-year history of the following symptoms:
- Urinary urgency and frequency
- Splitting of urine
- Urinary incontinence
- Post void dribble
- Groin pain that radiates into the penis (pelvic pain)
Josh also had decreased libido due to fear of urgency following intercourse and increased anxiety levels about his condition. Josh works full time, which requires him to enter and exit a work truck multiple times throughout the day, which would aggravate his symptoms and even cause urinary incontinence. Josh was an avid soccer player, winning championships in his career, which did lead to injuries including hamstring and adductor strains on several occasions. Josh now plays soccer recreationally but has stopped for several months due to worsening of his symptoms. Josh had seen multiple physicians over the years who told him he had prostatitis despite negative findings in urinalysis and blood tests. Josh was put on multiple rounds of antibiotics to “treat” his prostatitis, but none of which were helpful. Josh had to urinate every 5 minutes with only a few drops coming out at a time, which then led him to dig deeper into what he was dealing with. Upon discovering through his own research that pelvic floor muscles could be driving his symptoms, he stumbled upon Pelvic Health and Rehab Center and decided to seek treatment.
Josh’s Goals
- Determine if his pelvic floor muscles were the driver of his symptoms
- Decrease pelvic pain and discomfort (pain relief)
- Work a full day without urinary urgency interrupting
- Return to soccer
Physical Findings:
Upon physical examination, physical findings include myofascial restrictions to:
- Medial thigh hip flexors (iliacus)
- Deep hip rotators (obturator internus and piriformis)
- Gluteal muscles
- Myalgia and restrictions to the right ischiocavernosus and bulbospongiosus (some of our pelvic floor muscles)
- Difficulty performing a “pelvic drop”
- Difficulty relaxing his pelvic floor muscles after completing a pelvic floor contraction
- Decreased hip internal and external rotation mobility
Plan and Outcome
The findings listed above likely began following injuries to his right hamstrings/adductors and a lack of stretching and mobility over the years that was not prioritized during his soccer career. Beginning his job a few years ago led to increased stress and anxiety levels, likely exacerbating his physical symptoms to appear 3 years ago. We call this the “perfect storm”.
To start, I provided Josh with a home exercise program that included:
- Diaphragmatic breathing with pelvic floor drops
- Pelvic floor relaxation exercises to target his areas of restrictions and pain
- Happy baby pose
- Child’s pose
- Piriformis stretch
- Adductor rock backs
- Foam rolling to his inner thighs, hamstrings and glutes
After a few sessions, Josh began to notice a stronger urine stream and did not notice his symptoms worsened as much toward the end of his work day. On Josh’s 4th visit he reported he had a period of normalcy and only urinated 3 times during his work day whereas previously he had to go up to 20 times during his day.
Chronic Pelvic Pain Treatment included:
Manual therapy
including myofascial manipulation and connective tissue mobilization to UGT, medial thighs and deep rotators
Motor control training
to pelvic floor muscles to improve pelvic floor drops.
Education
on the nervous system’s involvement in the pain cycle
Reading
“Explain Pain” pages
Body scans
to bring awareness of increased clenching through the glutes and abdominals
Progression of Home Exercise Program:
- At home symptom management (massage gun, heat, stretch routine)
- Single leg strength training and stability to prepare for a safe return to soccer
- Dynamic warm up and cool down routine for soccer
Through Josh’s commitment to his home exercise program and consistency with physical and occupational therapy sessions, in 3 months he was able to have the confidence and ability to try soccer again, and in 4 months was playing symptom free, without fear and discomfort. Being able to be a part of his treatment team after getting his chronic pelvic pain diagnosed is something we are grateful for! Chronic pain can be tricky to diagnose without a multidisciplinary approach.
Josh’s Story:
My journey with Chronic Pelvic Pain Syndrome began in 2019 when one day I just had the urgent need to urinate more than 10 times per hour, sometimes going more than 60 times per day. As per usual my first instinct was to make an appointment with my doctor to determine the cause of it. After testing negative for bacteria with a urine culture I was told that I needed to take antibiotics and it left me wondering if this was necessary. I eventually took the first round of antibiotics and it did nothing, went back with my doctor and again after testing negative for bacteria in a urine culture I was given Bactrim and this seemed to do the trick because my urge was completely gone. Unfortunately they only helped for so long*, the symptoms eventually returned once more and it took a complete toll on my life as I was crushed mentally dealing with it. My Dr. told me there was nothing he could do at this point and referred me to a Urologist who eventually also prescribed an antibiotic, which was Cipro. After reading and researching on my own I decided not to take it because of the very bad side effects and also because I previously had taken other antibiotics with no great help or any help. At this point I was desperate to find a solution. On doing my own research I found that I could potentially have Chronic Pelvic Pain Syndrome and researched clinics around my area that would take me in. Unfortunately many do not treat men, but I was able to find Pelvic Health and Rehabilitation Center and they were able to take me in. They completely changed and gave me my life back. Upon finding that my urinary issues were due to Chronic Pelvic Pain Syndrome was a complete sense of relief because I knew I had finally found an answer to my problem. I had finally got the answers that I had been looking for.
My Chronic Pelvic Pain Syndrome originated from my early years of playing sports causing my muscles to tighten up as well as sitting for long periods at work and also due to stress. Cambria has been amazing at treating my condition, she is very knowledgeable in this and in any questions that may come up she has the answers. With her help and techniques that I have acquired from PHRC I have better outlook for the future knowing there is a solution to Chronic Pelvic Pain Syndrome. I will forever be grateful for the center for doing what they have done and continue to treat myself and other patients.
* The reason Bactrim temporarily helped Josh is because it is what is called a “broad-spectrum” antibiotic. When it is indicated people usually have a pain-causing infection and this medication includes an analgesic (pain reducing) component in addition to the antibiotic to fight the infection. This gives our patient the false sense that they have an infection because the analgesic may reduce their chronic pelvic pain symptoms while they are taking the medication.
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Did you know we opened our 11th location in Columbus, OH? Now scheduling new patients- call (510) 922-9836 to book!
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC PFPT via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.