
By Elizabeth Akincilar, MSPT, Cofounder, PHRC Merrimack
Pelvic pain is a complex condition that can have various causes, including medical conditions, injuries, and certain behaviors. In this blog, we will discuss 10 common behaviors that can potentially lead to pelvic pain(and potentially chronic pelvic pain). It’s important to note that while these behaviors may contribute to pelvic pain, they may not be the sole cause. Whether it’s acute pelvic pain or not, you deserved quality treatment and getting your pelvic pain diagnosed!
Understanding these behaviors can help you make positive changes to prevent or alleviate pelvic pain.
Constipation or straining to evacuate stool
Chronic constipation or frequently straining during bowel movements can put pressure on the pelvic floor muscles, leading to pain and discomfort.

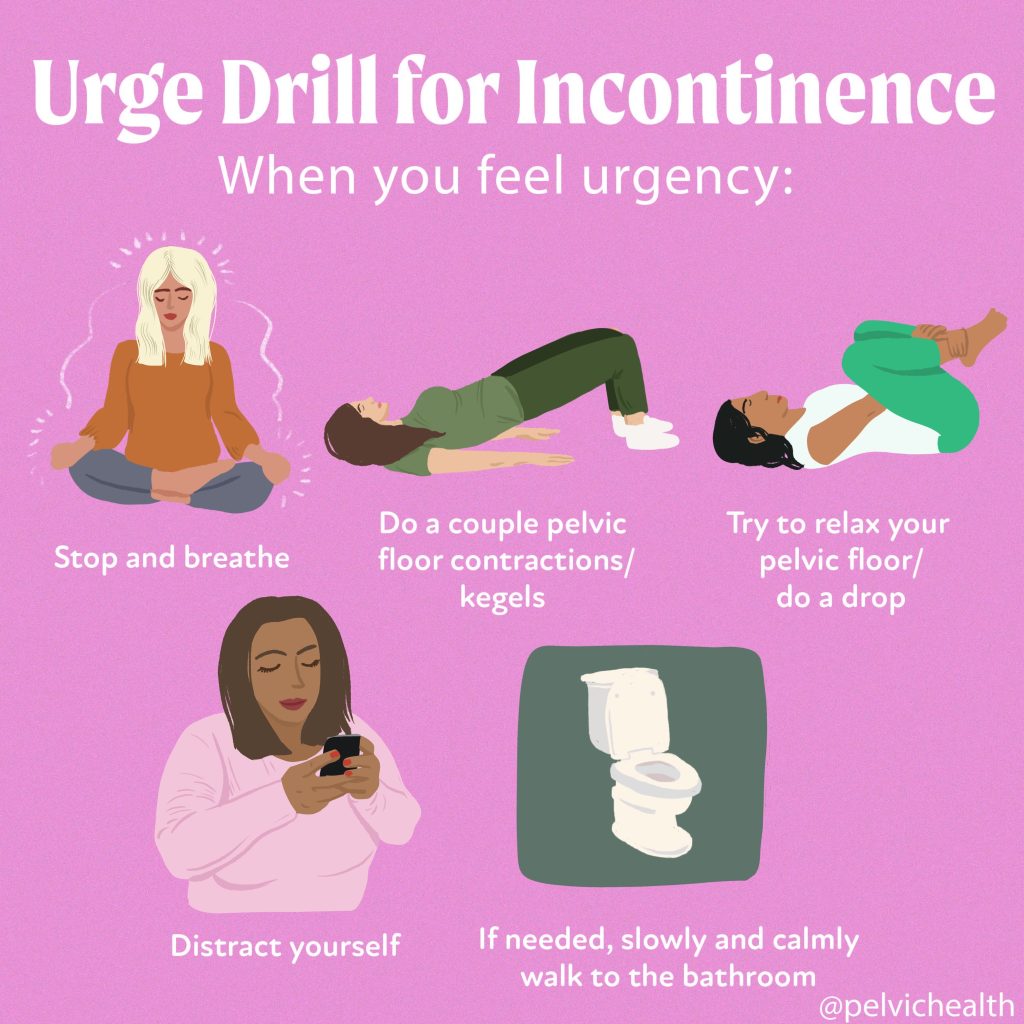
Holding your urine or delaying urinating
Ignoring the urge to urinate or frequently holding your urine can cause the bladder to become overactive and lead to pelvic pain.
Sitting all day
Prolonged sitting can cause the pelvic floor muscles to become tense, contributing to pelvic pain. Taking breaks to stand, stretch, or engage in light movement throughout the day can help alleviate this.
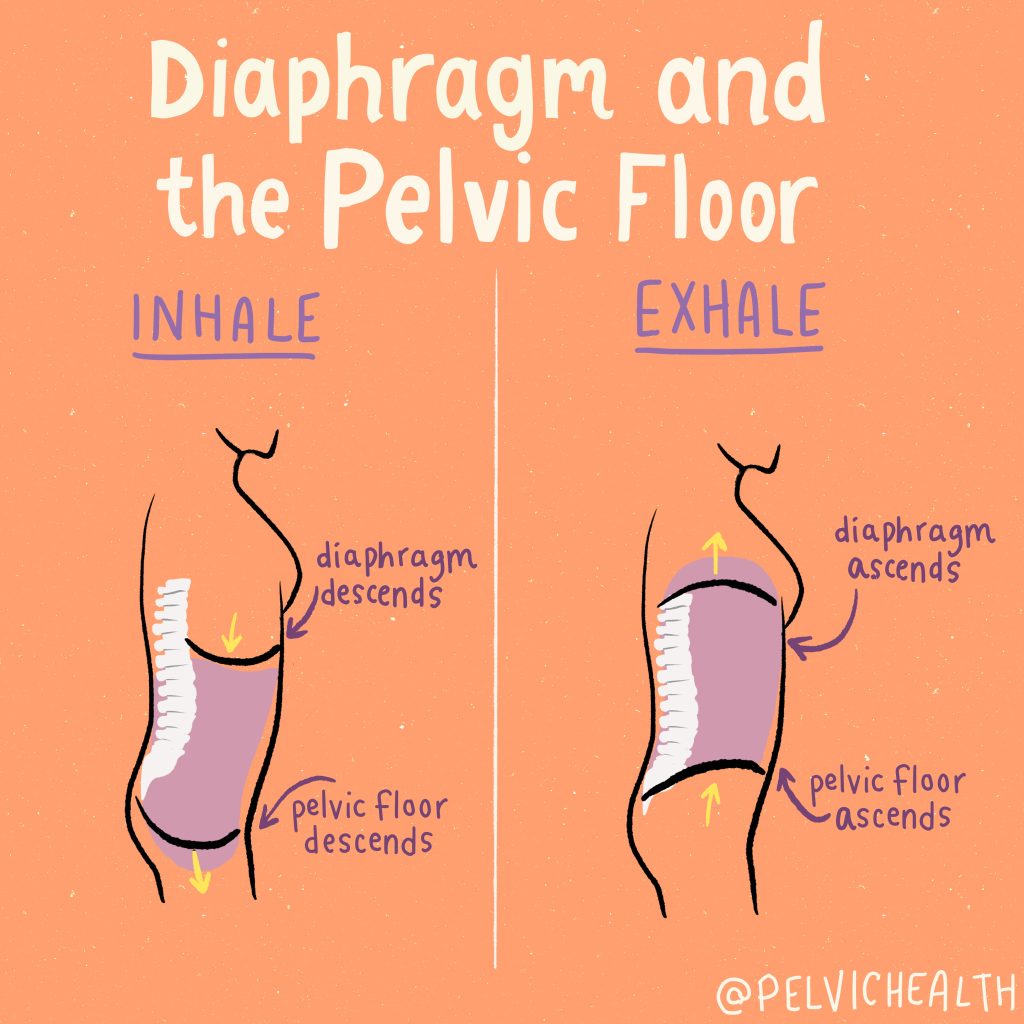
Holding your breath
Holding your breath during activities like lifting heavy objects or exercising can increase pressure on the pelvic floor muscles, potentially leading to pelvic pain. Focus on maintaining proper breathing techniques during physical exertion.
Clenching your butt
Habitually tensing or clenching your buttock muscles can put strain on the pelvic floor muscles, leading to pain and discomfort. Becoming aware of this habit and consciously relaxing your buttocks can help reduce pelvic pain.
Holding in your belly
Constantly holding in your stomach muscles can strain the pelvic floor muscles and contribute to pelvic pain. Practice consciously relaxing your abdominal muscles when not engaging in physical activity.
Incorrect breathing mechanics during weightlifting
Improper breathing techniques during weightlifting, such as holding your breath, can increase pressure on the pelvic floor muscles and potentially lead to pelvic pain. Consult with a professional to learn proper breathing techniques during exercise.
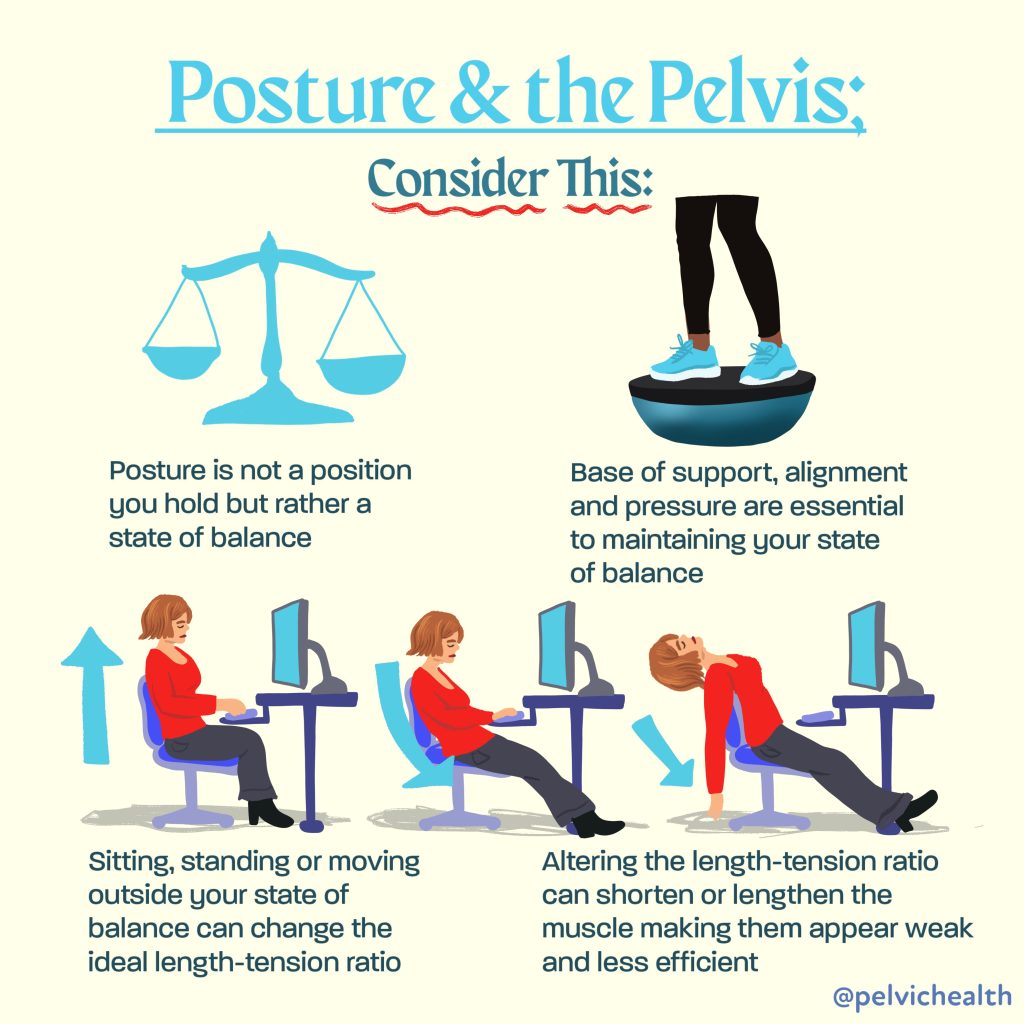
Postural dysfunction
Poor posture, such as slouching or hunching over, can affect the alignment of the pelvis and spine, leading to pelvic pain. Maintaining good posture and engaging in exercises that promote core strength and flexibility can help alleviate pelvic pain caused by postural dysfunction.
Edging during sexual activity
Edging, the practice of intentionally delaying orgasm during sexual activity, can cause the pelvic floor muscles to become tense, resulting in pelvic pain. Communicating with your partner and finding a balance that prevents excessive muscle strain can help prevent this.
Excessive or aggressive masturbation
Engaging in excessive or aggressive masturbation can strain the pelvic floor muscles and potentially lead to pelvic pain. Being mindful of your body’s limits and avoiding excessive or forceful stimulation can help prevent this.
It’s important to note that every individual is unique, and what may cause pelvic pain in one person may not affect another in the same way. If you are experiencing pelvic pain or discomfort, it is essential to consult with a healthcare professional, such as a physical and occupational therapists specializing in pelvic health, to properly diagnose and treat the underlying cause. They can provide personalized guidance and recommend appropriate treatment options to help alleviate your pelvic pain.
Remember, addressing these behaviors and seeking professional help can lead you on the path to pelvic pain relief and improved overall well-being.
Remember, addressing these behaviors and seeking professional help can lead you on the path to pelvic pain relief and improved overall well-being. Whether you are experiencing: chronic pelvic pain, pelvic inflammatory disease, painful menstrual cramps, irritable bowel syndrome, or other pelvic pain, help is available! Please check out our chronic pelvic pain resources below:
Resources:
How to find informed medical providers
International Pelvic Pain Society Find a Provider
International Society for the Study of Women’s Sexual Health
American Physical and Occupational Therapy Association’s Section on Women’s Health PT Locator
Herman and Wallace Find a Provider
Pelvic Guru Provider Directory
Have chronic pain but don’t know where to start? Get your pelvic pain treated today by requesting an appointment with us virtually to see how pelvic floor physical and occupational therapy can help you!
Frequently Asked Questions
Q: What are pelvic floor muscles?
A: The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
Q: What is pelvic floor physical and occupational therapy?
A: During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
Q: Do I need pelvic floor therapy forever?
A: The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Q: What other causes pelvic pain should I know about?
A: We recommend checking out our services to find a complete list!
______________________________________________________________________________________________________________________________________

Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.