
By Cambria Oetken, DPT, PHRC Westlake Village and Stephanie Prendergast, MPT, PHRC Pasadena
HOT off the Press:
Menopause is finally getting the attention it deserves in recent years with an exponential amount of attention in 2024. This year, Let’s Talk Menopause has considered their advocacy work, heading to Capital Hill and hosting in-person events for women. Tamsen Fadel and Denise Pines produced the documentary The M Factor which aired on PBS this October (stream it for free NOW!) and is being screened around the country.

While menopause was previously characterized as hot flashes and vaginal dryness, we now know so much more. This week we share new research about another symptom caused by hormonal decline: muscle and joint pain. While this sounds frustrating, understanding the role hormones play in our musculoskeletal health can be viewed as a therapeutic opportunity to help people live their best lives.
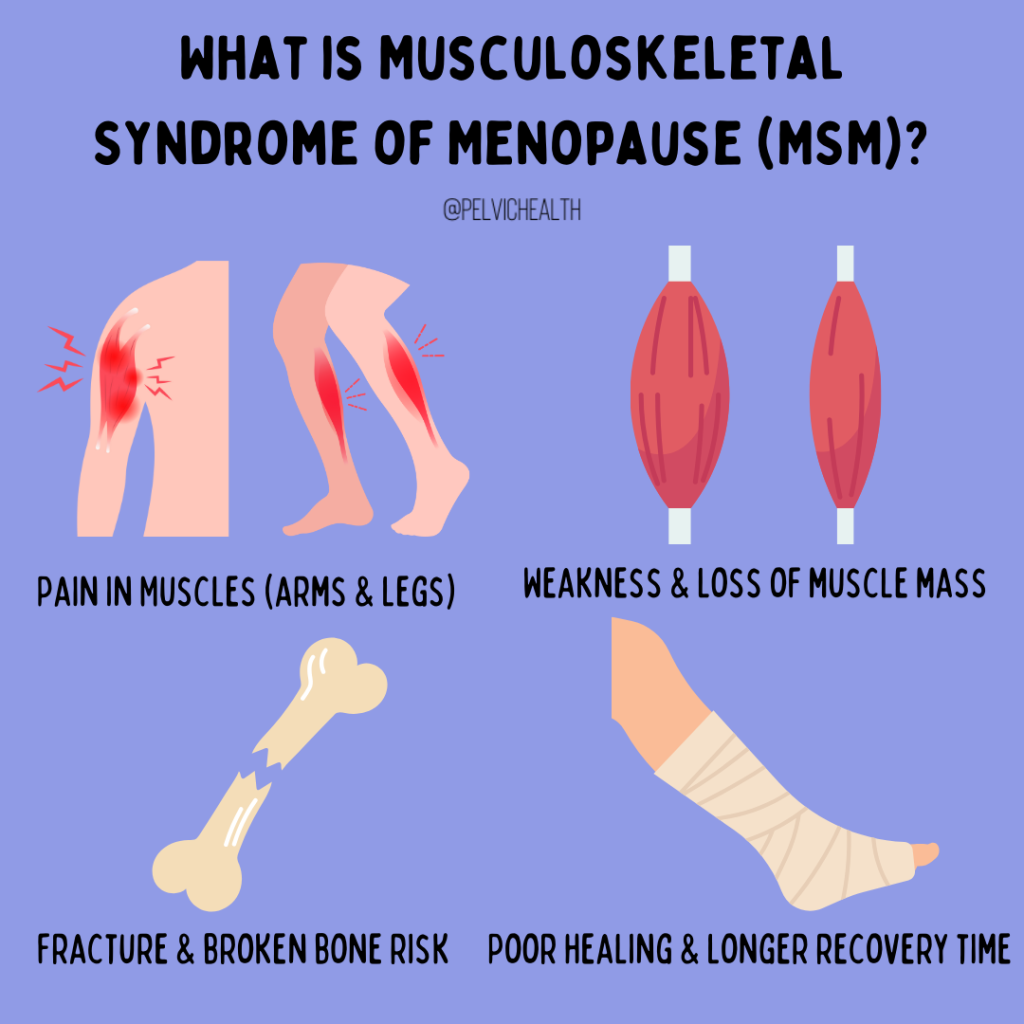
A recent article has introduced a new term called the Musculoskeletal Syndrome of Menopause (MSM) discussing the implications of menopause on our muscular system due to the precipitous drop in estrogen during this transition. Approximately 2 million women in the US will enter menopause annually, 70% of those women will experience the musculoskeletal syndrome of menopause, and 25% will experience severe symptoms. Menopause is considered a transition that occurs between the ages of 45 and 55 and has 35 known symptoms being associated with it. Menopause is typically determined as occurring 12 months after a woman’s last menstrual cycle, and can also be confirmed with additional lab testing. With the relevance of how many women experience menopause yearly it is crucial to be aware of the symptoms associated with it and how we can best treat these women to optimize their wellbeing.
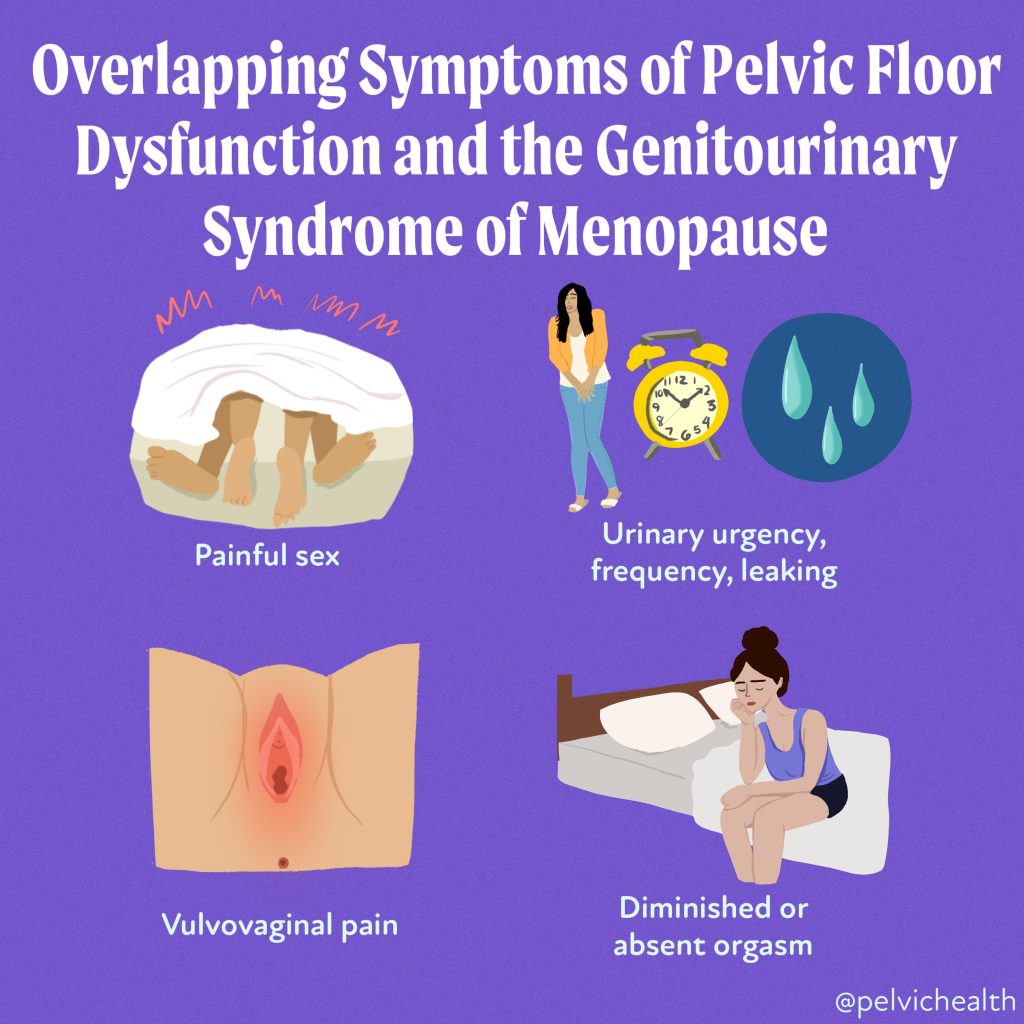
Common symptoms of menopause include hot flashes, brain fog, sleep disturbances, anxiety, menstrual changes, night sweats, vaginal dryness and more. A previous syndrome that has been recognized is the genitourinary syndrome of menopause (GSM) which has been presented in previous articles discussing the genitourinary symptoms that can occur.

The article discussed her states that the the musculoskeletal syndrome of menopause (MSM) includes, but is not limited to, musculoskeletal pain, arthralgia (joint pain), loss of lean muscle mass, loss of bone density with increased risk of resultant fracture, increased tendon and ligament injury, adhesive capsulitis (“frozen shoulder”), and cartilage matrix fragility with the progression of osteoarthritis. These musculoskeletal issues can be attributed to the decline in estradiol which is a fundamental form of estrogen needed for bone, tendon, muscle, cartilage, ligament and adipose.
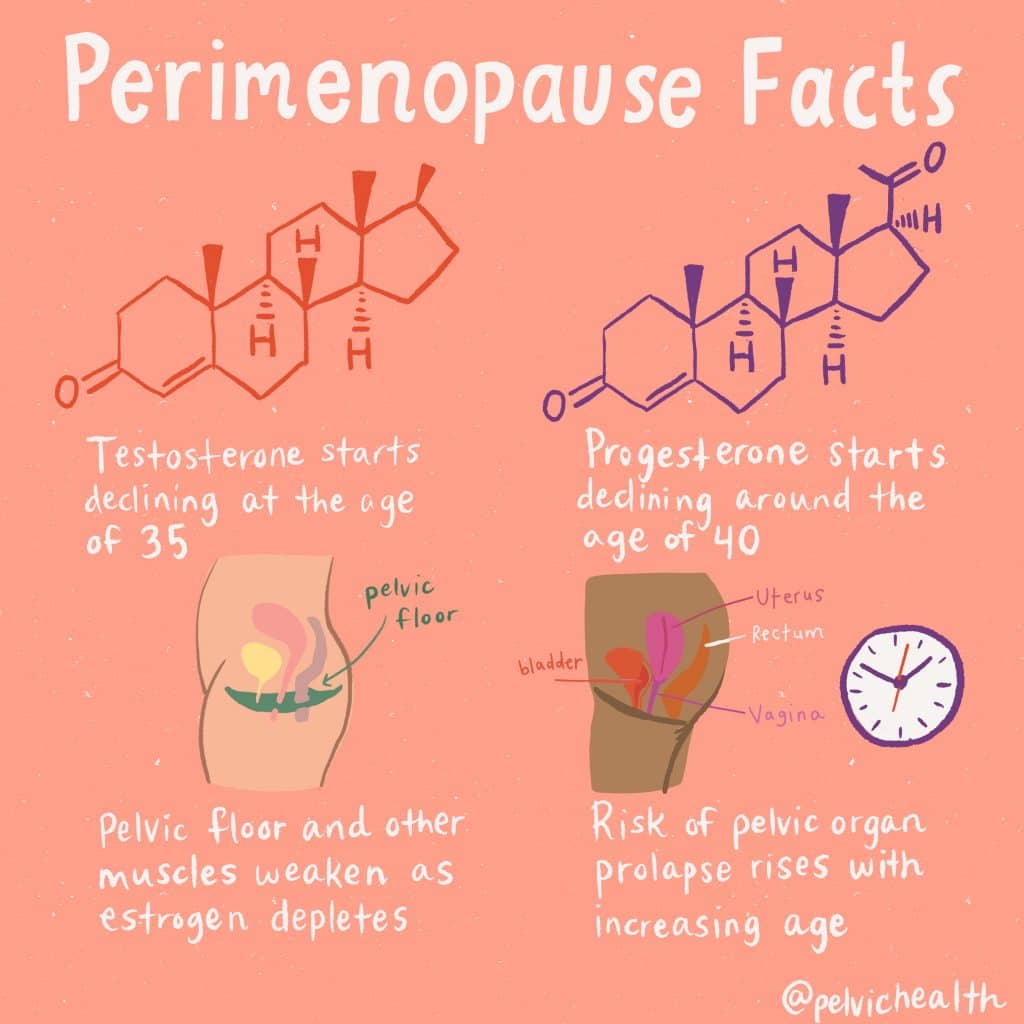
The decline in estrogen in perimenopause and menopause lead to 5 primary changes that will be summarized below.
1. Increased Inflammation
More than half of menopausal women report arthralgia or joint pain symptoms. Estrogen is a known inflammatory regulator that is part of our immune system and thus with this significant drop in estrogen, inflammation can become more difficult to combat. The article discusses menopausal hormone therapy (MHT) as an important treatment option to help regulate these symptoms of inflammation.
2. Sarcopenia
Sarcopenia is the age related loss of lean muscle mass with an increased amount of intramuscular adipose tissue (fat!). There are some nutritional interventions that have been recommended in the literature including protein, vitamin D and creatine that are shown to be effective in combination with resistance training. The decrease in estrogen is also an imperative factor associated with this condition that also decreases insulin sensitivity. With decreased estrogen capacity it can become difficult to regulate glucose especially in the skeletal muscle. The suggested method to assist in this long term is menopausal hormone treatment and resistance training.
3. Satellite Cell Proliferation
Satellite cells, also known as stem cells are crucial cells found in muscle fibers and are activated during an injury to repair muscle tissue. Estradiol is the hormone responsible for stimulating these cells to begin the repair mechanism. However, when we lose this stimulation that estrogen drives, muscle strength and recovery become impaired, making recovery from injury slower and less efficient.
4. Bone Density
You have likely heard of osteoporosis which affects 200 million menopausal women and is an underdiagnosed condition that is preventable and treatable! 30-50% of women will suffer a fracture in their lifetime which puts them at significant risk for long term chronic pain, disability and even death. Prevention of this is key and includes optimal nutrition, resistance training, and yep, you guessed it hormone treatment should it be appropriate. Hormone treatment has been shown to prevent and treat osteoporotic fractures.
5. Cartilage Damage and Osteoarthritis
There is conflicting evidence in the relationship between estrogen decrease and the frequency of hip, knee and finger osteoarthritis as well as the severity of hip osteoarthritis. However, estrogen has shown to have protective properties in the intervertebral discs of our spine which could suggest its role in helping to prevent osteoarthritis and further cartilage damage. Though more research is needed, there is pertinent evidence that estrogen replacement therapy can partake in reducing these changes in the connective tissue matrix.
The article considers the conservative approaches that are available should menopausal hormone replacement not be an option for certain patients. The study discusses the benefits of Vitamin D2 on bone turnover, magnesium to help optimize Vitamin D and K2 to potentially decrease the progression of and treat osteoporosis. Creatine and protein intake are also heavily studied nutritional options in improving bone mineral density and muscle power output.
Along with these nutritional supplements is resistance training, which is an accessible, non medical option that is a crucial component in managing musculoskeletal care, preventing age related injuries and decreasing mortality rates. Talking with your physical and occupational therapists in creating a safe, effective and progressive weight training plan can be utmost beneficial.
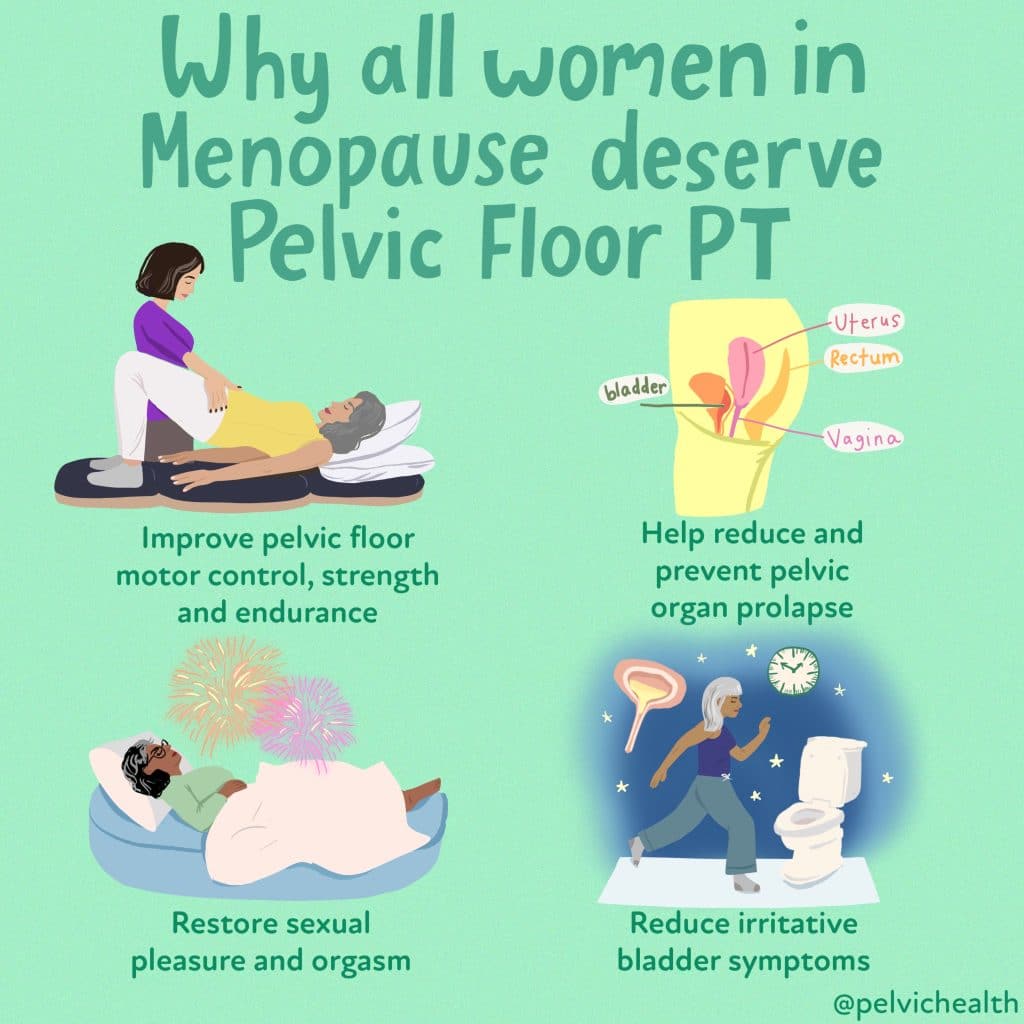
Pelvic Floor PT and MSM
Since resistance training has continued to be a recommended staple in the prevention of these major primary factors associated with MSM, your physical and occupational therapists can be a guide in navigating this long term. During a physical and occupational therapy examination your PT can evaluate your strength, ROM, pelvic floor strength, and functional goals you may have in order to develop a customized exercise plan to meet your needs. PTs are trained to identify imbalances or weaknesses that could predispose you to injury, such as poor posture or dysfunctional movement patterns. Resistance training requires progressive overload to build strength, which means gradually increasing the resistance or intensity of the exercises. However, it’s essential to do this at the right pace to avoid overtraining or re-injuring yourself, especially if you’re coming back from an injury.
Your physical and occupational therapists can help you determine when to increase the intensity of your exercises based on your progress. They will monitor your response to resistance training, adjusting the program to ensure you’re constantly improving without putting yourself at risk. Whether it’s increasing weights, reps, or sets, or incorporating more complex movements, your PT can help ensure that you’re progressing in a way that’s both safe and effective.
In conclusion
This article suggests the importance for patients and their medical care team to be aware of the changes that occur with menopause and recognize prevention approaches in order to optimize this population’s well being. The combination of informed and shared medical management and physical and occupational therapy can help people feel more comfortable in their bodies. We are now spending ⅓ of our lives in menopause and there is no need to suffer.
Resources
Wright, V. J., Schwartzman, J. D., Itinoche, R., & Wittstein, J. (2024). The musculoskeletal syndrome of menopause. Climacteric, 27(5), 466–472. https://doi.org/10.1080/13697137.2024.2380363
The M Factor which aired on PBS this October
Find a certified menopause healthcare practitioner in your area
Further reading about menopause
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Did you know we opened our 11th location in Columbus, OH? Now scheduling new patients- call (510) 922-9836 to book!
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
tags: menopause symptoms, menopause transition, muscle pain, hormone therapy, hormone replacement therapy, muscle aches, women’s health, menopausal transition