By Cambria Oetken, DPT, PHRC Westlake Village
Here is What You Need To Know!
This year new moms are finally getting the attention they deserve! We are excited to report our trusted sexual medicine experts coined a new term that describes the genitourinary hormonal deficiencies of lactating moms experience.
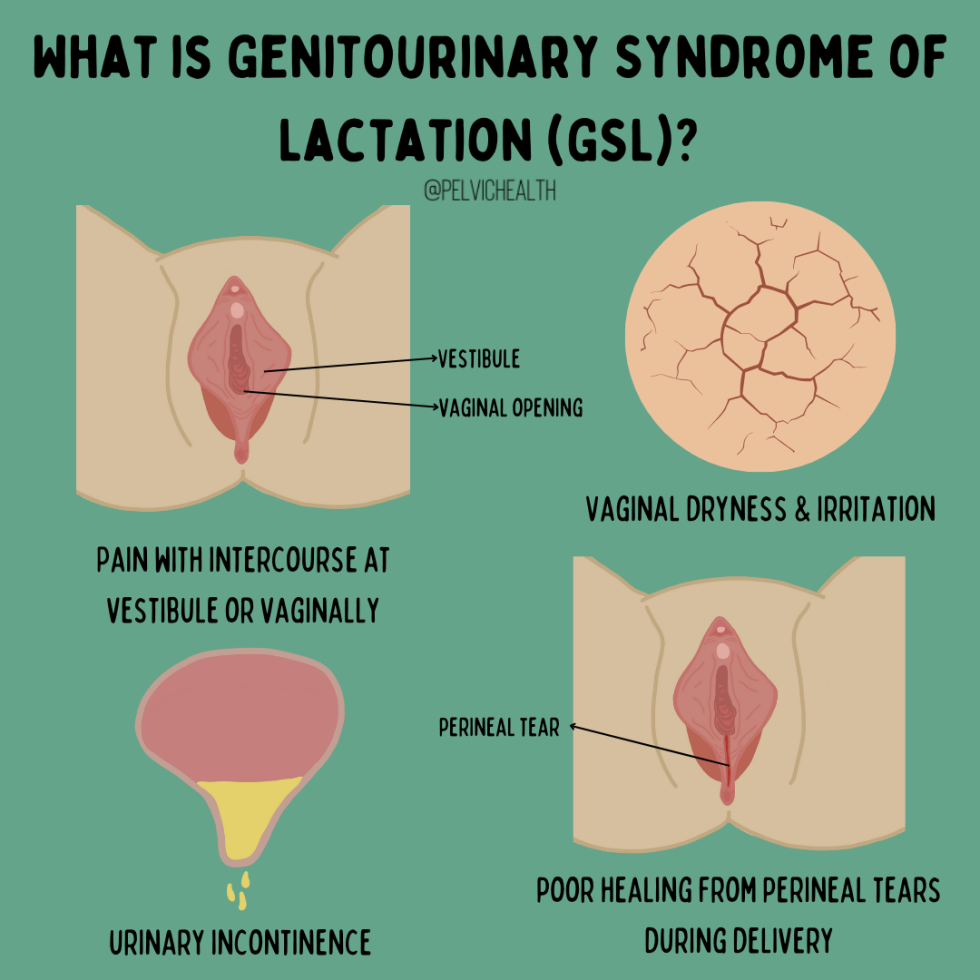
What is the Genitourinary Syndrome Lactation?
Earlier this year, an article was published proposing the novel term, genitourinary syndrome of lactation (GSL) in hopes to bring awareness to this population as well as the proper management, treatment and diagnosis. GSL describes the collection of genitourinary symptoms experienced by postpartum moms during the lactation period. While postpartum already encompasses significant changes both emotionally and physically, additional care should be provided for those suffering from genitourinary symptoms in order to alleviate burden and optimize wellness during a vulnerable time. The collection of genitourinary symptoms include vaginal dryness, dyspareunia, urinary symptoms and alterations in sexual function which can significantly impact these patients quality of life. This syndrome occurs due to hormonal changes associated with alterations in the genitourinary tract that will be discussed further.
Lactation and the potential impact on the genitourinary tract
Lactation comes with in depth physiological changes creating significant hormone shifts. In the first trimester of pregnancy, estrogen changes areola enlargement and maturation. In the second trimester, there is an increase in progesterone that helps with colostrum production and lobe proliferation. By the 3rd trimester, mature cells form, colostrum is produced by oxytocin in preparation for lactation to occur. Postpartum, there is a drop in progesterone and an increase in prolactin to drive milk supply. This increase in prolactin decreases the ovarian production of two crucial hormones, estrogens and androgens (such as testosterone). To maintain proper lactation, prolactin has to be present which in turn continues to suppress estrogen and androgen release. Lactating women therefore experience a hypoestrogenic and hypoandrogenic state, persisting at times as long as lactation continues. This state is similar to menopause. Estrogen is needed for maintaining vaginal wall thickness and lubrication as well as urethral and vulvar thickness. There are several estrogen receptors in this genitourinary tract including the clitoris and bladder trigone as well. Estrogen is also responsible for maintaining lactobacillus which is needed to maintain a healthy acidic PH to help fight off infections. Androgens also work hand in hand with estrogen to maintain vascularity and healthy vaginal tissue therefore, with the reduction of these, this puts the patient at risk for dyspareunia (pain with intercourse), Vestibulodynia (pain at the vestibule), and can limit sexual desire as a whole.

Vaginal dryness continues to be a primary concern in these individuals that can contribute to discomfort, irritation and pain with sexual intercourse (dyspareunia). Another contributing impact from a lack of estrogen is the ability to recover optimally from vulvovaginal tears or injury. Estrogen promotes growth of crucial cells to help repair tissue. Studies have shown that supplementing with estrogen can improve wound healing synthesis and boost collagen during this repair phase.

Another disrupting symptom that is common postpartum is urinary incontinence. Urinary incontinence is common postpartum and can be emotionally distressing and shameful for patients and society has normalized this as a result of pregnancy. Additional conditions include pelvic organ prolapse and even anal incontinence. There is a connection between SUI and collagen and as we know, collagen is reduced in lactating women due to depletion of estrogen needed for tissue repair and collagen optimization.
Treatment Approaches for Genitourinary Syndrome Lactation (GSL)
Pharmacological Options
Vaginal Estrogen Therapy can be an option for women experiencing vaginal dryness or with complaints of dyspareunia, recurrent UTIs, or vulvar and vaginal changes. While there are limited studies on estrogen therapy in this population, there have been positive subjective reports of improvement at the perineum with no serious adverse events noted. The concern and hesitation with vaginal estrogen use is that it may transfer to breast milk or reduce milk supply. However, even in studies using the highest dose of estrogen possible there were no traces of estradiol detected in breast milk and is unlikely to affect breast milk supply. We know from previous research that low dose vaginal estrogen is considered safe even in women with estrogen receptor positive malignancies (cancer).
DHEA has been indicated for the use for the genitourinary syndrome of menopause and is FDA approved for severe dyspareunia in postmenopausal women. DHEA works to convert to estrogen and testosterone and has limited concern for absorption systemically. DHEA is not currently being used in lactating mothers and there are a lack of studies in its use with this population.
Non pharmacological Options
Functional Microablative CO2 laser is being studied for vulvovaginal atrophy and some researchers have found improvements in dyspareunia, pain at vaginal orifice and dryness.
Vaginal Lubricants and Moisturizers
Lubricants and moisturizers can be helpful in this population as vaginal dryness tends to be one of the most common concerns that can also impact sexual functioning. This option could be a first step approach that is conservative and easily accessible. Moisturizers and lubricants with hyaluronic acid (HA) have been shown to significantly improve these symptoms and even quality of life just after 12 weeks of use. Additional studies have shown HA use with estriol cream to have an even greater impact when combined. Some of our favorite moisturizers and lubricants can be found below.

Pelvic Floor Physical and Occupational Therapy and Occupational Therapy
This is crucial in optimizing both peripartum and postpartum challenges involving the genitourinary tract. Through exercises, manual therapy, education on proper postures especially with breastfeeding, body mechanics, improving pelvic floor motor control and strength, enhancing sexual wellbeing and overall optimizing postpartum recovery. Therapy can also help to reduce severe perineal tearing through instruction on perineal massage and positional options during delivery to further reduce recovery time postpartum. Pelvic floor therapy has been shown to decrease the risk of urinary incontinence in late pregnancy and postpartum and women were less likely to report pelvic organ prolapse and with a reduction in unsatisfactory sexual function. Pelvic floor therapy should be considered standard care during and after pregnancy to optimize function, well being and prevent potential genitourinary symptoms.
Conclusion
In conclusion, GSL hopes to be recognized as a diagnosis to help bring support and optimal treatment to these lactating individuals in order to optimize their well being both emotionally and physically during a critical period. Should you be an expecting mom, reaching out to your physical or occupational pelvic floor therapist is a great start to begin preparing for progression of pregnancy, delivery and postpartum and can help guide you through an evolving time. Therapists can also work closely with your provider in managing GSL. If you live near one of our 11 locations, please give us a call, we are happy to help!
Reference:
Perelmuter S, Burns R, Shearer K, Grant R, Soogoor A, Jun S, Meurer JA, Krapf J, Rubin R. Genitourinary syndrome of lactation: a new perspective on postpartum and lactation-related genitourinary symptoms. Sex Med Rev. 2024 Jun 26;12(3):279-287. doi: 10.1093/sxmrev/qeae034. PMID: 38757214.
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
tags: genitourinary system, urinary tract, breastfeeding, birth, infants, support, breastfed, health