Lessons Learned & Future Hopes
By Jandra Mueller, DPT, MS, PHRC Encinitas
Once a year, in March, individuals – providers, advocates, and patients, dedicate their time to promoting education around increasing awareness about Endometriosis. Though for many of us, we are just becoming louder during this time, hoping our efforts will expand further. We are in a moment where our country is facing many uncertainties when it comes to ‘women’s’ healthcare, and without many answers. For this week’s blog, and in honor of Endometriosis Awareness Month, I’d like to take a moment and reflect on lessons learned and experiences gained as both a patient and as a provider and share my hopes for the future direction of care for those suffering from Endometriosis.
What is Endometriosis?
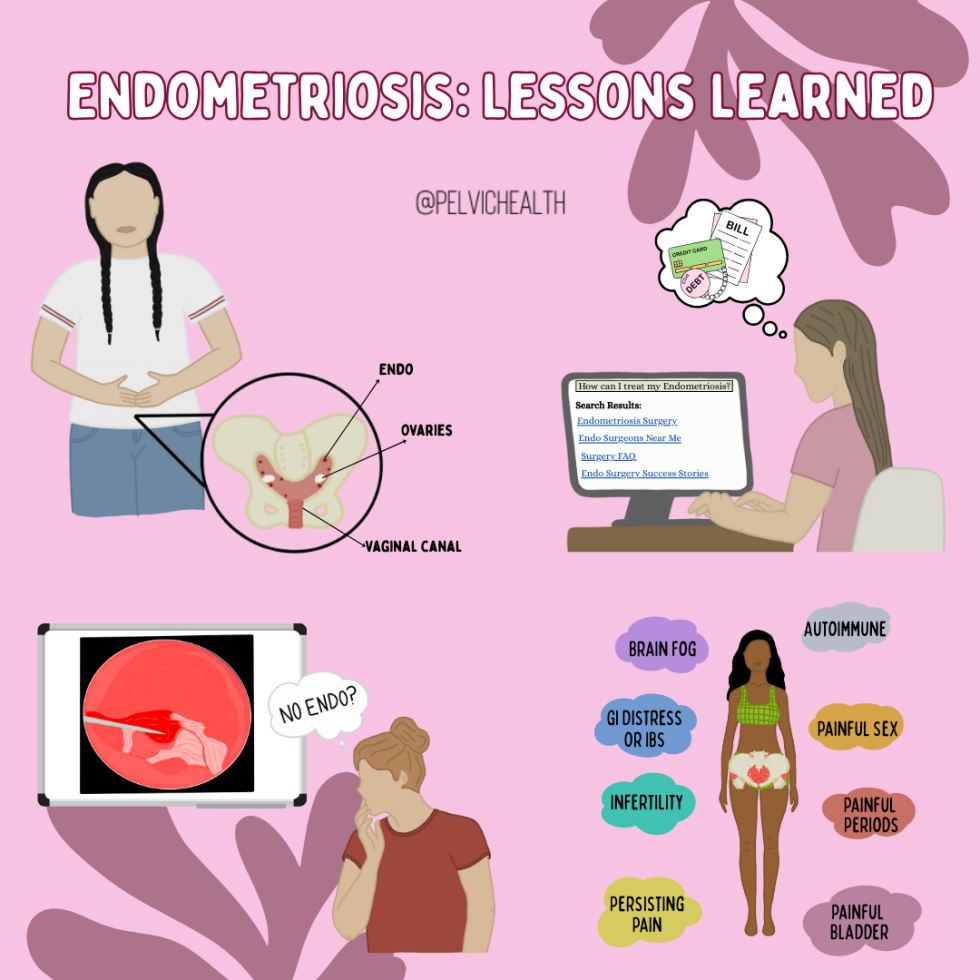
Endometriosis is a heterogenous, estrogen-dependent, inflammatory disease characterized by the presence of endometrial-like tissue found outside of the uterus, primarily in the abdominopelvic cavity and ovaries as well as extra-pelvic sites.
Lesson #1: The definition of endometriosis matters. Why?
When endometriosis is defined as “endometrial tissue found outside of the uterus” this implies that endometriosis is the endometrium. While endometriosis lesions and the endometrial lining share similar histological (cellular/tissue) characteristics and behave similarly in some ways, these are different tissues; in fact, these tissues do not always show the same cellular components and do not always respond to the same treatments. Over the years, more research and education campaigns have adopted this updated terminology, but it is likely you will still see endometriosis defined this way.

Using this outdated terminology reinforces that endometriosis is all about the uterus. The focus of research, the use of medications, and surgical procedures are aimed at the uterus and stopping growth of the endometrium and menstruation. The result is that the emphasis for treatment are birth control pills or inducing a state of menopause either temporarily with medications or permanently with a hysterectomy. Not only has this focus impacted how providers approach the care for those with endometriosis, this thought process has influenced our guidelines for treatment and management and insurance coverage may only cover these types of treatments.
Lesson #2: Provider and Patient Goals Do Not Always Align and Here’s Why
This is a hard one for medical providers and advocates alike because we feel so strongly about how care should be approached and what the ‘right’ way is. This was a hard pill to swallow and one of the biggest causes of division in the endometriosis community in my opinion. Having gone through a very long delay in getting the care I needed, with many wrong answers and encounters with providers lacking the in-depth knowledge I needed to receive the care that helped me, I never want a patient to struggle with that.

While medications and ablation surgeries are not excision surgery, they are tools that can be beneficial when someone may not be in a place to get surgery – whether that is due to access, financial concerns, other health conditions, or simply that it isn’t the right time in their life, everyone has a right to choose their own path and what works best for them.
While I am, and will remain an excision advocate, I have come to understand that to be a good provider, advocate, and to build trust in my patients I need to put my own bias aside. The best way I can do that for others is to listen to them, thoroughly inform them about all of their options, what to expect with various medications, the benefits and drawbacks of various surgical approaches, why I approach care the way that I do, and offer support and guidance in their journey. In approaching care this way, I have found that my patients have been more comfortable asking questions without feeling shamed or isolated and ultimately receiving the care they deserve.
My Story
I was a pelvic floor physical and occupational therapists long before I knew I had endometriosis. My passion for endometriosis care grew because of my situation and the difficulties I had in getting the care I needed. What really inspired me to do more was the realization that if it was this hard for me, in one of the best positions to be able to navigate this, how on earth are people that are not in the medical field ever going to find answers? Well, it’s no surprise that so many people suffering with endometriosis often do know more about this disease than most medical providers.
Initially, the symptoms that led me to seek medical care were not the classic presentation of severely painful periods or infertility. It was abdominal bloating, intermittent severe pain resulting in ER visits from ‘rupturing cysts’ and severe constipation. I was 28 years old at the time, and my first excision surgery was when I was 31 years old. That is a three year gap, much lower than the average delay of 7-10 years. However, my symptoms started at age 13 shortly after starting my period. After a severe pain episode landing me in the ER, followed by the recommendation to start birth control, I had some reprieve from my symptoms until I no longer could control them. That is almost a 20 year delay in diagnosis. While birth control helped the recurring rupturing cysts and I could avoid the ER, what did not change was the severe dyschezia (one of the clinical manifestations of endometriosis) that would happen often and made me terrified of social activities.
My first surgery, a diagnostic lap, that my doctor agreed to do after a four day hospital stay was disappointing. I didn’t have endometriosis. There were some findings, and I love the doctor I worked with – she did listen to me, gave me options and told me her limitations. Our agreement was that she would only excise lesions she found (not ablate them) in areas she felt comfortable and she would take a lot of pictures.
While I never received a formal diagnosis after that, there were in fact findings – my left uterosacral ligament was ‘very odd’ and there was fluid in my pelvis. Turns out, the pathology showed ‘cells consistent with endometriosis’ in the fluid sample. Still no diagnosis. I also felt worse than I had prior to that surgery, none of the tools I’d found to help manage my symptoms were working to get me back to that pre-surgical baseline.
Luckily, I had resources that allowed me to have an excision surgery with a top surgeon in the months following where several areas were excised – most of which came back as some sort of fibrotic type tissue but a few that were clearly marked “endometriosis.” My surgeon told me that while these areas aren’t being flagged as endometriosis, they are, just a different form. The relief I had following that surgery was immediate and shocking.
Lesson #3: Fibrotic endo is endo.
This has become a huge area of interest for me when it comes to endometriosis research and managing patients who are still suffering. In 2022 I ended up having a second endometriosis excision surgery after a significant event ramping up inflammation and what we believe to be mast cell activation syndrome (MCAS). Once again, it was a huge success. Again, all the tissue that was excised came back as fibrotic tissue – which I found really interesting as there was significant overlap in both endometriosis and mast cell disorders, especially when it came to fibrosis and fibrotic endo.
To receive a confirmed diagnosis of endometriosis, tissue needs to be removed during surgery (excised/biopsied) and sent to the pathology lab and show the presence of ‘endometrial glands and stroma.’ Meaning, it needs to look similar to the endometrial lining. Fibrotic tissue does not have the endometrial glands and stroma so it is not considered endometriosis by definition, nor is it always removed during an excision surgery because of this reason. In a 2018 publication by Vignano et al., the authors urge that lesions demonstrating endometrial stroma and glands may not be the only relevant lesions. They argue that this process of injury and repair that is involved with fibrosis, may lead to fibrotic tissue instead of the typical lesion progression. This means that it may not be “old” endo that is irrelevant, but there may be other factors involved that lead this tissue to transform quicker, thus being missed during surgery.
A colleague of mine and I were asked to present at a mast cell conference in September 2024. Based on some research I had done, I am hypothesizing that mast cells have a role in this presentation of endometriosis. While researching for this talk, I had found that mast cell activity does in fact play a role in fibrosis and in endometriosis pathology, and in recent years, more attention has been looking at the role of mast cells in conditions such as neuroproliferative vestibulodynia and endometriosis. What I found most interesting, ‘adhesions,, a thin filmy tissue that can be present during surgery, and is also related to fibrosis, does not have presence of endometrial stroma and glands, but is one of the criteria in the endometriosis staging system.
Lesson #4: Excision surgery can mean many things.
Several years ago, I’ve found that when doing your due diligence and inquiring about different surgeons’ approach, excision or ablation, an excision surgeon was the whole package. Meaning, a thorough and detailed search was performed, and all abnormal tissue was removed. In recent years, I am finding this is not necessarily the case, and a big factor has to do with the fibrotic tissue that may be present.
After my experience with this, and having patients present to PT following surgery without relief, I started approaching the care of my patients differently. I would ask to look at their surgical pictures and read their surgical reports. One of the main issues I found was that fibrotic tissue was being missed. While some patients had ablative surgeries, many would state that they had an excision surgery. I’d refer them for a second opinion to a surgeon I was confident understood the implications of fibrotic tissue, and I’d get confirmation and patients started getting better.
Lesson #5: A technically successful surgery does not always mean it was clinically successful.
This is another extremely important lesson I’ve learned and is another tough one for patients as well as providers. Persistent pain following excision surgery does not always mean you had a failed surgery. Endometriosis is a very complex disease, and the presence of other conditions is higher, and can make recovery more difficult. There are several reasons someone with endometriosis can experience pain or other symptoms, beyond the lesions themselves. While eliminating the lesions is important, we cannot forget about the other pain generators. Whether symptoms are from another health condition, associated with endometriosis, or due to various treatments to help the symptoms of endometriosis, they all need to be identified and addressed.
Lesson #6: Pelvic Floor Evaluation is necessary but not currently included in the standard of care
Pelvic floor and girdle dysfunction, including muscle myalgia, myofascial trigger points, and signs of central sensitization are present in almost 90% of people with biopsy-confirmed endometriosis. Symptoms such as painful sex, irritative bladder symptoms, constipation, and pelvic pain are associated with endometriosis but also pelvic floor and girdle dysfunction. Finding a pelvic floor physical and occupational therapists is crucial as they can help you identify and treat the remaining factors or refer you to specialists who can help. Endometriosis requires a multidisciplinary approach that rarely ends at surgery.
Future Hopes
Medicine is always evolving and we are constantly learning more. My hopes for the future are that we can better understand this disease, learn more about the various presentations and how to approach care in an individualized approach. Below are some of the questions I hope we will have more information and solutions to in the future.
- Why does birth control really help some people and not others?
- Can we find new medications that are not solely focused on putting women into menopause but that may actually help treat a larger problem that is driving endometriosis?
- Can we find better, non-invasive diagnostic tools that are accessible and can aid in not only reducing the delay in diagnosis, but get people into surgery faster and support the need for better insurance coverage for excision surgery?
- Can we have a more standardized approach to surgery and management, better research addressing the nuances of surgery and medications, and better guidelines to drive insurance reimbursement?
Beyond this, I hope that the community as a whole can recognize that we are after the same goal: better care and accessibility for those to seek help. We can be diligent in our efforts to push for excision surgery while recognizing individualized care for each person – whether that be diet and lifestyle changes, medications, self-care, and of course a proper surgery. More now than ever, as a community we need to come together to push for change and recognize the impact on our patients, friends, loved ones and colleagues, without isolating others who prioritize different aspects of the care process.
Virtual and In Person Services at PHRC
We offer both in-person services and virtual. The physical and occupational therapistss at PHRC have undergone extensive continuing education to best help people with endometriosis. Often people do not understand their symptoms until they stumble upon our website, blog, or social media channels. Some people have a diagnosis but they do not have a pelvic floor physical and occupational therapists locally to help them. Other times people have a pelvic floor physical and occupational therapists but for some reason are not getting better or feel stuck in their treatment plans. Others just want another opinion from trusted experts. Whatever your individual needs are, we are here for you and ready to help!
Jandra Mueller of PHRC Encinitas developed the first course for physical and occupational therapistss to help patients manage their care more effectively and successfully.

Jandra recently teamed up with iCareBetter, an endometriosis advocacy group, to start Endometriosis Unplugged, a podcast dedicated solely to endometriosis.
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
tags: pelvic pain, chronic pelvic pain, menstrual periods, scar tissue, menstrual cycle, endometriosis diagnosed, menstrual blood, bowel movements, painful menstrual cramps, treatment of endometriosis, abdominal pain, treat endometriosis, diagnose endometriosis, chronic disease