By Alexa Savitz, DPT, PHRC Pasadena
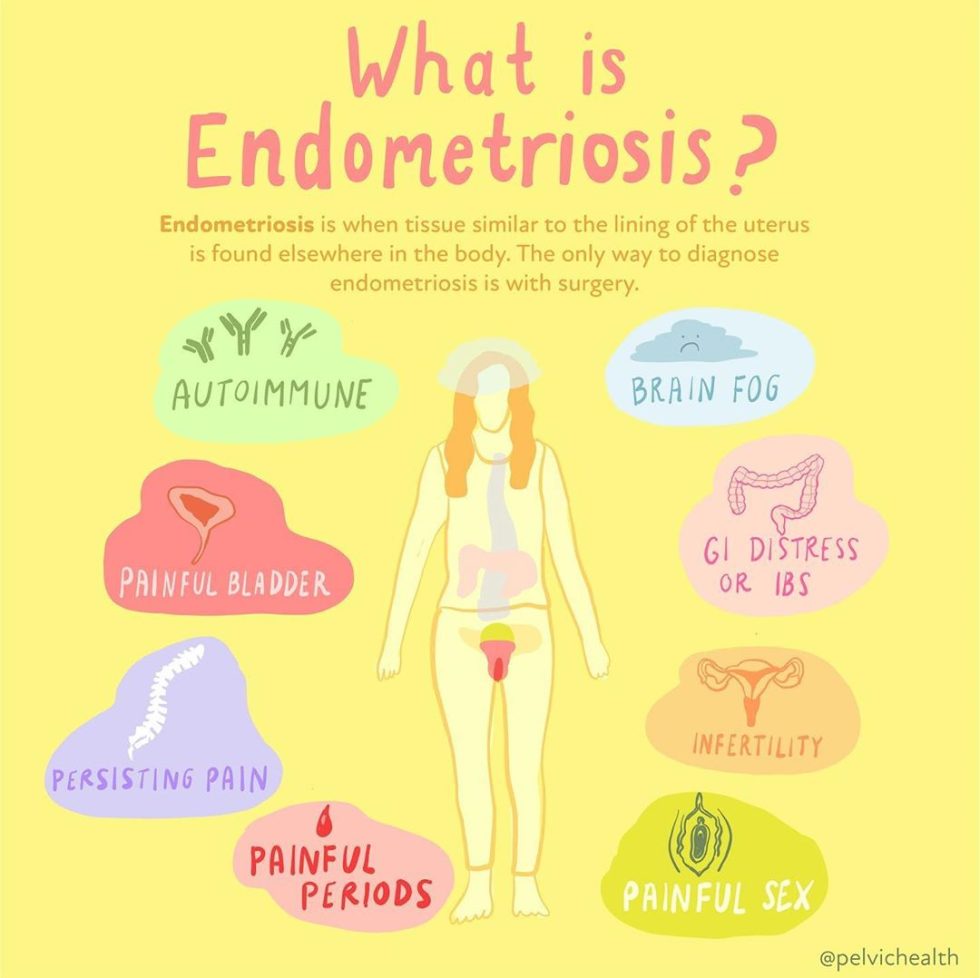
Endometriosis is a chronic inflammatory disease that is mediated by estrogen and can present as cyclic/non-cyclic pelvic pain, low back pain, GI and IBS symptoms, painful sex , infertility, painful bladder symptoms, fatigue and chronic pain, to name a few. The gold standard for diagnosis is laparoscopic excision surgery with histological confirmation.
While the goal of surgery is to remove all of the disease, a surgery that is a ‘technical’ success does not always result in resolution of all symptoms. There are several considerations as to why symptoms persist despite ALL of the lesions being removed. Some of the common reasons pain persists following surgery include the success of the surgery which involves the skill and training of the surgeon, identification or visualization and excising of all lesions, and the presence of other pain generators that have not been adequately addressed. Even with a perfect surgery, endometriosis can recur and pain can persist.

Patients are often recommended to use hormonal suppressants for symptom management, suppress the growth of new lesions, or prolong the time between surgeries with adequate symptom management. That being said, hormonal suppressants are almost always suggested before someone even gets to surgery. Oftentimes, when individuals report their symptoms to their doctor, surgery is almost never the first suggestion. Instead, current guidelines recommend pharmacological (medical) management as a first resort, these are known as first-line therapies. Medications such as birth control pills and anti-inflammatory medications can be helpful for many to reduce symptoms, but these options do not treat the actual disease. Moreover, when these medications fail, many providers will suggest more aggressive forms of hormonal suppression; while some people report improvement in symptoms, they come with significant side effects and more often than not, are a short-term solution to managing symptoms of endometriosis at best.
As our friend and colleague Rachel Rubin says
“You can’t mess with hormones without understanding the consequences.”
This is absolutely true for those with endometriosis when the majority of those suffering from this disease, or symptoms of this disease, are given medications that are focused on shutting down, or altering estrogen levels.
As pelvic floor physical and occupational therapistss, we have a role in not only managing the musculoskeletal and nervous system for our patients, we are often the ones helping them navigate their journey with this disease. Because we have the benefit of spending ample time with our patients, we have the ability to spend the time educating them about their symptoms, provide resources, and help navigate the complexities of the health system .
While pelvic floor physical and occupational therapistss cannot and do not prescribe medications, we do see the impact these medications have on one’s pelvic health and sexual well-being. We believe you should also know what to look for in order to have an educated conversation with your healthcare providers to find the best solution for you.
Medications for Endometriosis and Impact on Pelvic & Sexual Health
We understand that finding the right surgeon can be difficult; some individuals do not want surgery and would rather use medications for management. Regardless if you choose this option or the reasons why, informed consent is absolutely necessary to make a decision. That also means knowing the impact on your pelvic and sexual health.
The four primary groups of hormonal medications used for those with endometriosis are:
Combined Oral Contraceptives (COCs)
Progestins
Gonadotropin releasing hormone agonists (GnRH-agonists)
Gonadotropin releasing hormone antagonists (GnRH-antagonists)
Combined Oral Contraceptives (COCs):
- Contains both synthetic estrogen and progestin and orally administered
- Typically lower costs
- Frequently used for dysmenorrhea (painful periods)
- Reduces menstrual flow, menstrual and pelvic pain
- Can be used continuously which may be more effective than cyclic use (placebo pills)
- Further research is needed to determine their efficacy in managing pain associated with endometriosis.2

Progestins:
Progestin only (no synthetic estrogen)
- Various forms available including oral pills aka ‘the mini-pill,” the implant, hormonal IUDs, injections (medroxyprogesterone acetate aka the Depo-Provera shot).
- Tend to be better tolerated, lower adverse effects and research shows they are preferred in cases of endometriosis for symptom management and potentially slowing progression of the disease.
- The proposed mechanisms of action according to research:
- Decreasing follicle stimulating hormone (FSH) and luteinizing hormone (LH) resulting in anovulation (no ovulation) and a hypoestrogenic state
- Some research suggests a direct impact on the endometriosis lesions by reducing growth (proliferation), reduced inflammatory response by provoking apoptosis of these cells, and inhibiting angiogenesis (the growth of new blood vessels that fuel lesion growth).2
- Side effects can include irregular uterine bleeding or spotting, weight gain, mood changes and depression, and bone loss.



GnRH-agonists:
Subcutaneous muscular injection (daily, monthly, in 3-6 month intervals)
- Proposed mechanisms include:
- Stimulate the release of LH and FSH from the pituitary gland in the first 10 days.
- The spike in LH And FSH creates a feedback loop which downregulates GnRH receptors causing a decrease in LH and FSH.
- These changes create a suppression of estrogen and induce amenorrhea (no period).
- Endometriosis symptoms may increase initially due to the surge in LH and FSH.
- No longer routinely used as new drugs have come on the market
- Has been shown to increase pregnancy by 4-fold, so it is often used in cases of infertility.
- Side effects include amenorrhea, vasomotor symptoms, sleep disturbances, accelerated bone loss, urogenital atrophy.
- It is still under FDA review for increased risk of cardiovascular disease and diabetes.
GnRH-antagonists:
Has essentially replaced the GnRH agonist for use in endometriosis
- Administered orally
- Proposed mechanisms
- Acts to suppress GnRH production by competing with endogenous GnRH for its pituitary receptors suppressing LH and FSH resulting in a rapid modulation of circulating estradiol levels.
- The effect on modulating estradiol is dose dependent.
- Does not provoke an initial flare up like GnRH-agonist
- Side effects include hypoestrogenism and genitourinary syndrome of menopause symptoms despite the dosage (i.e. decrease bone density, hot flashes, increased serum lipid levels).
- Non-hormonal contraceptives should be used as pregnancies have occurred.
Potential Consequences of Hormonal Suppressive Therapies
Where hormonal suppressive therapies do have their place in the overall care for individuals with endometriosis, nothing comes without consequences. The above-mentioned pharmacological treatments are focused on the same result: stopping ovulation and menstruation; ultimately, putting individuals in a hypoestrogenic state, essentially medical menopause.
Symptoms associated with menopause or low estrogen states such as vasomotor symptoms (hot flushes/flashes), mood fluctuations, vulvar irritation, pain, dryness, low libido and arousal, UTI-like symptoms are all possible with these medications, even in your 20’s. Conditions associated with a low estrogen state such as Vestibulodynia and Genitourinary Syndrome of Menopause (GSM) encompass the local impacts depletion of hormones can have on the genitourinary structures.


Individuals with endometriosis are at a significant risk for developing these symptoms since guidelines suggest that these medications are a crucial part of disease management. These medications do have a role and many people have found them to be extremely helpful in managing symptoms and living their lives, but are often not told about the impact they can have on their pelvic and sexual health.

Painful intercourse (dyspareunia)
is one of the most common manifestations of endometriosis and one of the most common consequences of pelvic pain and hormonal suppression. When endometriosis is the culprit, we are referring to deep dyspareunia or pain with deep thrusting, because the innervated lesions are being provoked or there is scar tissue, etc. Entry pain or superficial dyspareunia, is also common in those with endometriosis, but endometriosis lesions are not the direct cause. More likely, the medications used to ‘treat’ endometriosis are the culprit.
That being said, pelvic floor dysfunction (PFD) and the pelvic floor muscles can also be a cause of both deep and superficial dyspareunia; and many people with endometriosis often are dealing with all three causes.

Painful urination (dysuria)
is another common clinical manifestation of endometriosis. While endometriosis lesions on the bladder, PFD, dietary factors, gut issues, mast cell activation syndrome and histamine are common factors, hormonal deficiencies also are a common reason people will experience this symptom. Commonly, people report a history of chronic UTI’s or UTI-like symptoms, many times with a negative culture along with urinary frequency or urgency. They may have even received a diagnosis of interstitial cystitis/painful bladder syndrome (IC/PBS). Along with vulvar dryness, painful sex, urinary symptoms such as these are common with Vestibulodynia and GSM.
The vestibule is made up of the same tissue as our bladder and surrounds the urethra. When this tissue is irritated, or inflamed, due to friction from penetrative intercourse, an ultrasound probe, speculum, or even tight clothing, it may present as urinary frequency, urgency, pain with urination or these UTI-like symptoms.


In Conclusion
The delay for diagnosis of endometriosis is 7-10 years, many of these symptoms are present and either misdiagnosed and/or dismissed either by the provider or even the patient themself. The impact these symptoms have on the pelvic floor is huge, further contributing to PFD and pelvic pain.
The management of endometriosis takes a village and a multidisciplinary approach. It is important to both address the disease itself, the endometriosis lesions, identifying and addressing the additional pain generators such as myofascial pain, pelvic floor dysfunction, the central nervous system, normalizing local hormonal deficiencies, and overlapping visceral inflammation contributions.
Birth control and other hormonal suppressants may play a role, and for some, the critical component to managing their disease and living their life. As physical and occupational therapistss it is important to understand the role we play in helping patients understand this disease and all of the components involved, including the impact their medications may have on their pelvic health. Seeking an evaluation from a pelvic floor physical and occupational therapists trained in sexual medicine and pelvic pain is an important step to help you get the help you need.
We are key players on the team and can help you facilitate communication between your healthcare providers and refer you to the appropriate providers that can get you the treatments you may need. Being informed about the treatment options you have is important and together we can help you navigate endometriosis and achieve your goals.
References:
Stratton P & Khachikyan I, et. al. Association of Chronic Pelvic Pain and Endometriosis with Signs of Sensitization and Myofascial Pain. Obstet Gynecol. March 2015; 125(3): 719-728.
Vannuccini S, Clemenza S, Rossi M, Petraglia F. Hormonal treatments for endometriosis: the endocrine background. Rev Endocr Metab Disor. 2022. 23:333-355.
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Did you know we opened our 11th location in Columbus, OH? Now scheduling new patients- call (510) 922-9836 to book!
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok