By Stephanie Prendergast, MPT, Cofounder PHRC Pasadena
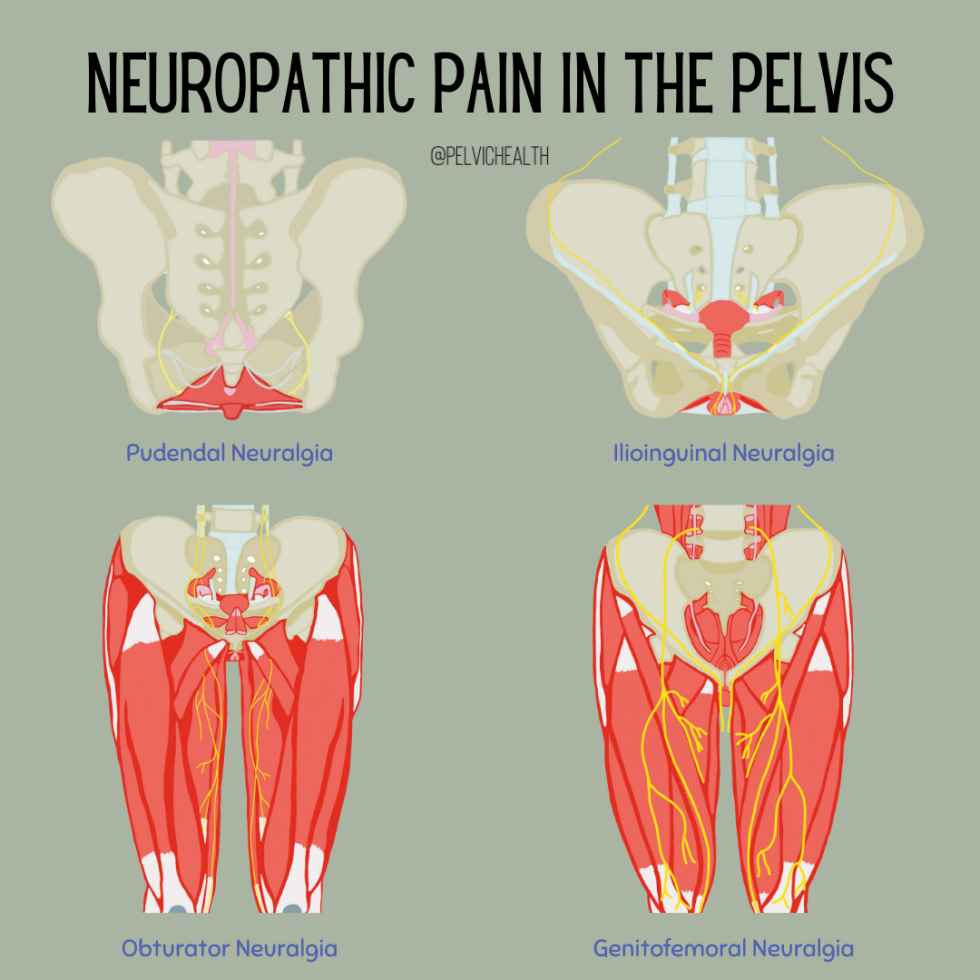
Many people experiencing burning in their pelvis or pain while sitting may google their symptoms and quickly arrive at a diagnosis of Pudendal Neuralgia. The pudendal nerve is an important pelvic nerve, however, the ilioinguinal nerve, the obturator nerve and the genitofemoral nerves can also cause pelvic pain and should not be overlooked. It is crucial to have a proper diagnosis in order to get relief and that starts with anatomy and physiology!
Starting with the basics, the term neuralgia simply means pain in the territory of the nerve. Any nerve can turn into neuralgia if it gets compressed, over stretched, or otherwise injured through surgery or trauma.
Peripheral nerves are responsible for sensation and movement. When injured, neuropathic pain can result. Symptoms of neuropathic pain include burning, tingling, shooting, stabbing, jabbing, itching, numbness, pain reaction to non-painful stimuli (allodynia), and exaggerated reactions to painful stimuli (hyperalgesia), and altered reactions to temperature.
It often surprises people to learn that most neuralgias are diagnosed simply based on the characteristics and locations of the pain. Electrophysiologic testing and imaging techniques are not as helpful as we would like them to be for making a diagnosis. The most important information our patients tell is their (suspected) mechanism of injury, exactly where the pain is and exactly what it feels like.
Let’s define the 4 important pelvic nerves to consider in order to differentially diagnose pelvic neuropathic pain. Please note there are more nerves to consider and some people can have multiple neuralgias at the same time.
Pudendal Neuralgia
The pudendal nerve contains autonomic, sensory and motor fibers. The autonomic component of the pudendal nerve distinguishes it from the other three nerves in this blog post. The autonomic nervous system is designed to keep us functioning automatically without us thinking about it. The pudendal nerve contributes to urinary, bowels and sexual functioning in addition to its sensory and motor features. This nerve has a lot of pelvic responsibility!
Definition
Pudendal neuralgia consists of stabbing, burning pain in one, some or all of the areas the pudendal nerve nerve innervates. These areas include the vulva (clitoris, labia minora/majora, inner labial area, vestibule), penis, scrotum, perineum, urethra, anus and perineum. This nerve innervates the pelvic floor muscles and is reflexively involved with sexual arousal and orgasm, and urine and stool storage and release. Pudendal neuralgia pain tends to get worse when sitting, squatting, and with trunk or hip flexion. The majority of people with pudendal neuralgia also have pelvic floor dysfunction and pain, peripheral nerve sensitivity in other nerves such as the posterior femoral cutaneous and sciatic nerves, and dysregulation of the central nervous system.
Causes
Pudendal Neuralgia can be caused by several different scenarios The most common include:
- Tension injuries: examples include constipation, childbirth, squatting exercises with faulty mechanics
- Compression injuries: examples include bike and horseback riding, prolonged sitting, faulty sitting mechanics
- Surgical trauma: examples include pelvic organ prolapse repair, obstetric injuries, hip surgeries
- Biomechanical abnormalities/movement pattern abnormalities of the lumbo-pelvic-hip complex and lower extremities
Treatment
Skilled pelvic floor physical and occupational therapy and medical management are the key to effective treatment of pudendal neuralgia, a successful treatment plan usually involves multiple interventions. The right medical team can help you determine which interventions will be most helpful and when to implement them. The entire team at PHRC specializes in the management of PN and frequently helps patients form the right medical team and decide on appropriate interventions.
Physical therapy involves manual therapy, pain science education, a home exercise program, modification to your current exercise program, and guidance with lifestyle modifications.
Because we treat a large volume of people with pudendal neuralgia at PHRC we have created a Resource List with blogs, videos, and reputable materials. PS – we are also working on a Pudendal Neuralgia e-book, make sure you subscribe to our newsletter and follow us on social media to get the e-book when it’s released!
Ilioinguinal Neuralgia
The ilioinguinal nerve is a sensory and motor nerve. Ilioinguinal neuralgia can be confused with pudendal neuralgia because both nerves can cause nerve pain in the labia and penis. The primary difference between ilioinguinal neuralgia and pudendal neuralgia is that ilioinguinal neuralgia may cause pain in the inguinal canal (groin) whereas pudendal neuralgia will not. The pudendal nerve does not innervate the groin. People with ilioinguinal neuralgia may have (nerve) pain with sitting and this is one reason why people may understandably think they have pudendal neuralgia, however, if the anatomy does not match up it is likely not PN.
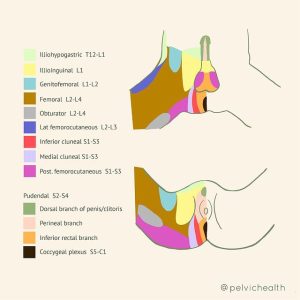
Want to see more images like this? Check out our Dermatome blog!
Definition
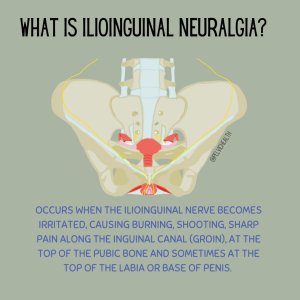
Ilioinguinal neuralgia occurs when the ilioinguinal nerve becomes irritated, causing burning, shooting, sharp pain along the inguinal canal (groin), at the top of the pubic bone and sometimes at the top of the labia or base of penis.
Causes
Inguinal hernia or inguinal hernia repairs, pubic symphysis trauma or separation, surgical trauma, scar tissue (ie Cesarean scars).

Treatment
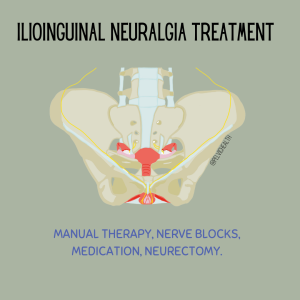
Physical therapy, nerve blocks, medication, hernia repairs if present, neurectomy.
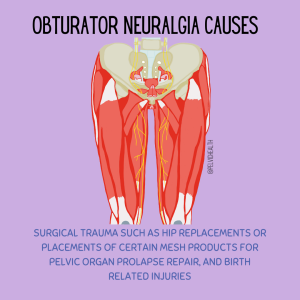
Obturator Neuralgia
The Obturator Nerve is a sensory and motor nerve. It can be confused with pudendal neuralgia because both will typically cause pain with sitting. However, the obturator nerve does not innervate the genitals and it can cause aching in the pubic area, groin, and upper medial thigh. Another difference between obturator neuralgia and pudendal neuralgia is that obturator neuralgia will also cause pain in the upper inner thigh whereas pudendal neuralgia will not.
Definition
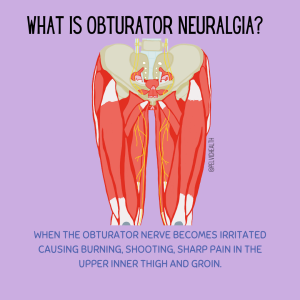
When the obturator nerve becomes irritated causing burning, shooting, sharp pain in the upper inner thigh and groin.
Causes
Surgical trauma such as hip replacements or placements of certain mesh products for pelvic organ prolapse repair, and birth related injuries
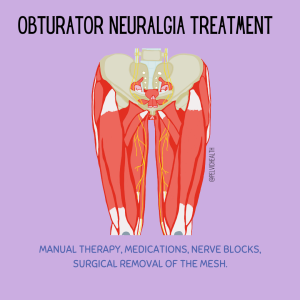
Treatment
Manual therapy, medications, nerve blocks, surgical removal of the mesh.
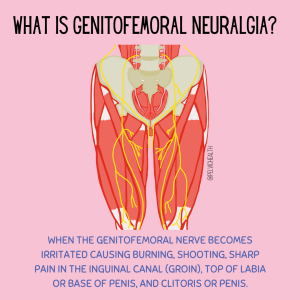
Genitofemoral Neuralgia
The genitofemoral nerve is a sensory and motor nerve. Genitofemoral Neuralgia can be confused with pudendal neuralgia because both nerves can cause pain in the clitoris and penis! The primary difference between genitofemoral neuralgia and pudendal neuralgia is that genitofemoral neuralgia is going to cause pain in the inguinal canal (groin) whereas pudendal neuralgia will not.
Definition
When the genitofemoral nerve becomes irritated causing burning, shooting, sharp pain in the inguinal canal (groin), top of labia or base of penis, and clitoris or penis.
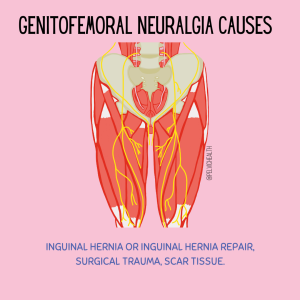
Causes
Inguinal hernia or inguinal hernia repair, surgical trauma, scar tissue.
Treatment
Manual therapy, medications, nerve blocks, neurectomy.
Take Home Points!
- Any peripheral nerve can suffer injury and a neuralgia can develop
- A diagnosis for neuralgia can be made by understanding the character and anatomic location of the pain
- A physical examination by a doctor or physical and occupational therapists can help identify neuralgias in a clinical setting, sometimes imaging and/or electrophysiological testing may help the diagnosis
- A combination of skilled physical and occupational therapy and medical management leads to successful treatment!
If you are experiencing severe pain and you believe it is due to pudendal neuralgia, trigeminal neuralgia, or any type of pelvic pain, it’s time to check in with a pelvic floor physical and occupational therapists. Pain relief is possible with the right treatment plan and a multidisciplinary approach. Chronic pelvic pain is no joke! We understand the depths of severe pain at PHRC and pelvic floor physical and occupational therapy can be a part of your treatment plan.
Have more questions? Check out a short Q&A below!
Q: What can happen if Ilioinguinal neuralgia is left untreated? Should I be worried about my spinal cord or nerve pain?
A: If a neuralgia is left untreated, the pain could get worse and could also affect surrounding structures as your body tries to compensate due to the pain. We would recommend seeking treatment if you suspect that you have a neuralgia (whether it’s pudendal neuralgia or not).
Q: Is Ilioinguinal neuralgia common in pregnancy?
A: Ilioinguinal neuralgia can occur during pregnancy. We would recommend speaking with your OB/midwife if you suspect this and also working with a pelvic physical and occupational therapists.
Q: Is Ilioinguinal neuralgia hard to diagnose? What should I tell my doctors so they can test me extensively for it?
A: It can be difficult to diagnose and it is recommended to work with a pain management specialist to help further diagnose it as they are the ones most often prescribing the medication or performing the nerve blocks so they are more accustomed to common symptoms and ways to alleviate and treat the issue. Imaging may not show anything as this may be more functional versus an actual compression or entrapment. Nerve blocks can both be diagnostic and treatment. For example, if you have a nerve block and it reduces the pain that is important. Further treatment/ evaluation may be warranted if the pain returns, but it may be considered a positive diagnostic block.
Q: Can obturator neuralgia affect the hamstring as well? What nerve pain should I be looking out for?
A: Genitofemoral neuralgia primarily presents with pain in the genital region and sometimes the inner thigh, stemming from damage or irritation to the genitofemoral nerve. This pain can be sharp, shooting, or burning and may be accompanied by sensations like tingling or numbness, often triggered by activities such as walking or changing positions. On the other hand, obturator neuralgia is characterized by deep, aching pain in the inner thigh, occasionally radiating to the knee, caused by compression or injury to the obturator nerve. This condition may also lead to difficulties in adducting the thigh (bringing the thigh towards the midline of the body) and a sensation of tingling or numbness along the inner thigh. Both conditions share some overlapping symptoms, such as (nerve) pain and altered sensations, but they differ mainly in the location of the pain and the specific activities that exacerbate it.
Q: Is it possible to have both Pudendal Neuralgia and Genitofemoral Neuralgia? Do you have resources for nerve pain? I know pelvic pain can be tricky to diagnose (nerve pain being so close together).
A: Yes, it is possible to have both pudendal neuralgia and genitofemoral neuralgia.
Q: Many people have benefited from a TMS/ mind-body approach to PN, myself included. Do you aim patients towards those resources? (Mindfulness is only a small part of it.)
A: For anyone dealing with chronic pain, exploring the TMS/MindBody approach can be a worthwhile step. While mindfulness is an important component, the comprehensive strategies include identifying stressors, journaling, cognitive behavioral therapy (CBT), and sometimes engaging in physical activity against the instinct to avoid movement due to pain. We work with our patients through a multidisciplinary approach, so any referrals for other aspects of care are always given (when deemed appropriate for their case).
Stay tuned for a more in depth Q&A coming next month! Drop your nerve pain or pelvic pain related questions in the comments to have your questions answered in future Q&As!
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Did you know we opened our 11th location in Columbus, OH? Now scheduling new patients- call (510) 922-9836 to book!
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok