By Alexa Savitz, DPT, PHRC Pasadena
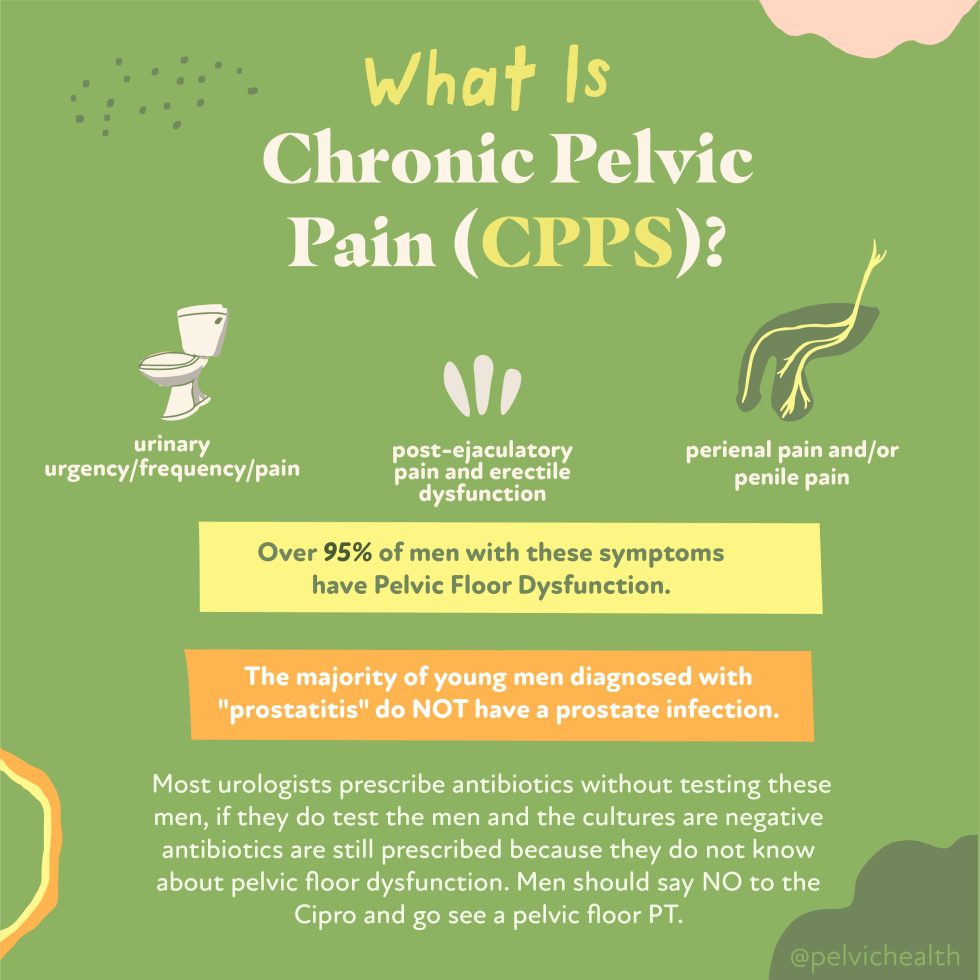
At PHRC we are no strangers to working with male pelvic pain patients. About 50% of our case loads at PHRC can be made up of male pelvic pain diagnoses. Research shows that up to 16% of men suffer from Chronic Pelvic Pain Syndrome (CPPS) at some point in their life. Pelvic floor physical and occupational therapy (PFPT) is an integral part of treating CPPS yet many people do not realize this. Here is a success story and case overview of how PFPT helped a male patient overcome CPPS.
Chris is a 32 year old who was referred to PHRC by a local urologist because of the following symptoms:
- painful urination
- urinary urgency and frequency
- pelvic pain with sitting
- pain with sexual function
He reported he had dealt with these symptoms for 1 year. Chris is a pilot and long trips multiple days per week required him to sit with this discomfort. You could imagine how his symptoms were impacting his quality of life.
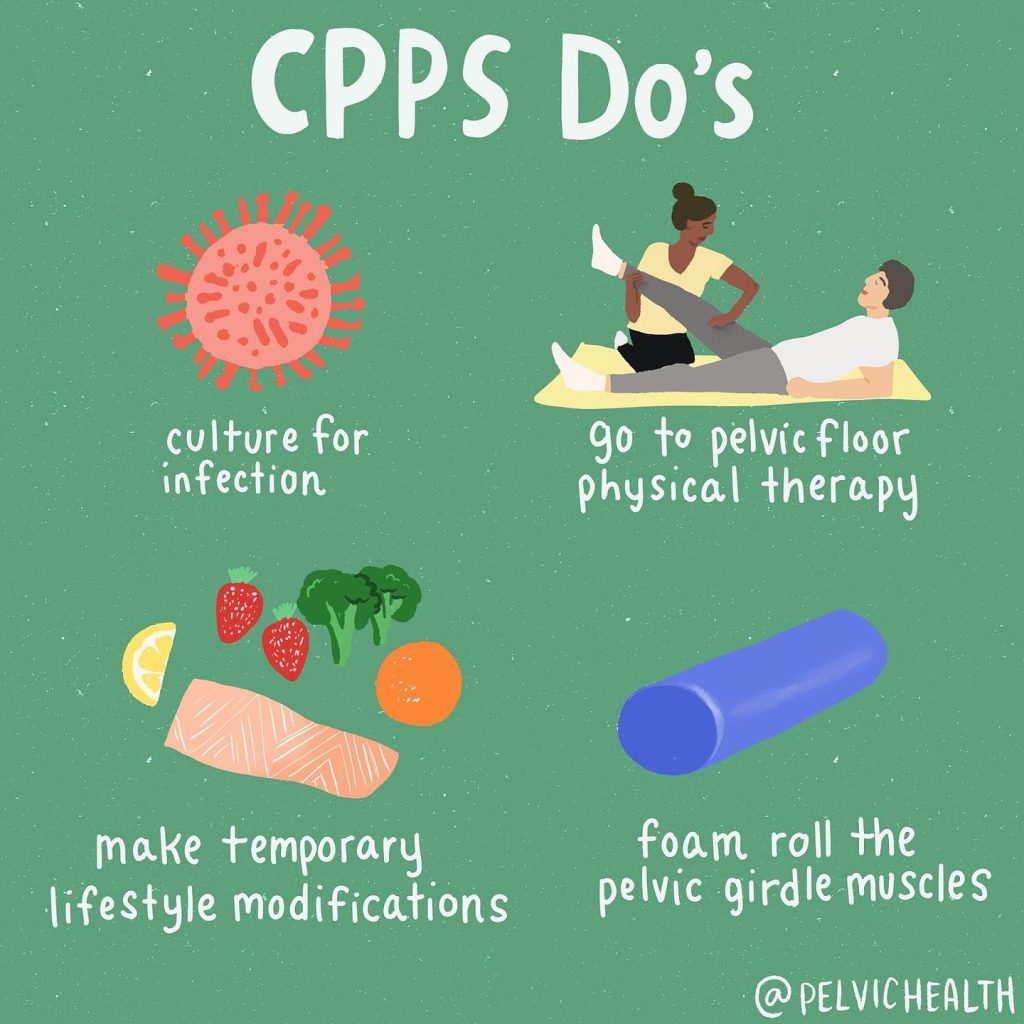
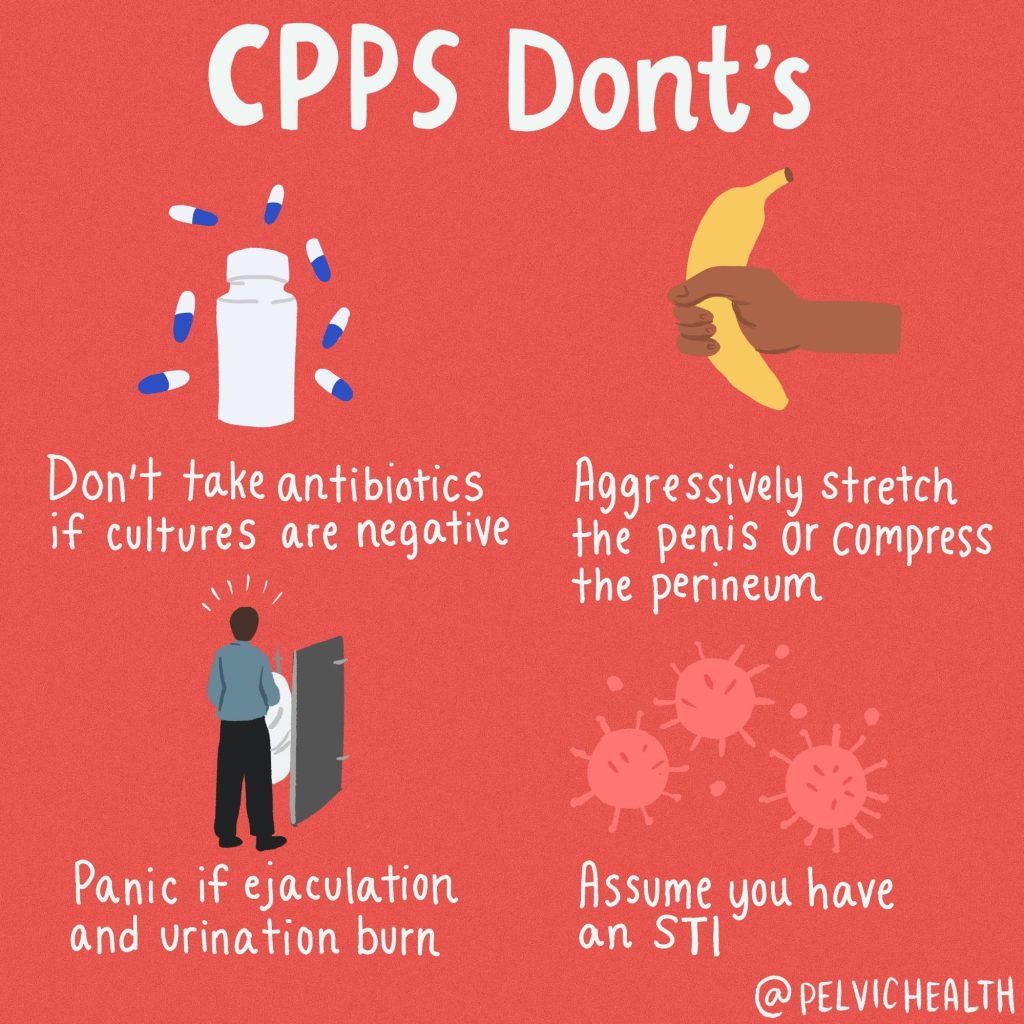
He had seen multiple providers, taken antibiotics, and had many tests performed including ultrasounds and CT scans that were all normal. He had begun eliminating bladder irritants including spicy foods and alcohol as he noticed these substances increased his urinary urgency and frequency. He tried eliminating coffee, however this was challenging to exclude from his daily routine and schedule, and he observed that it was associated with his urinary symptoms. Prior to coming to PHRC he started to use a cushion while sitting and had been doing pelvic floor stretches which helped jump start his journey towards healing.
Patient Goals:
Chris’ goals were to improve his pain and symptoms to make work travel more tolerable with less discomfort and to improve his pain associated with sexual function.
Physical Examination Findings
- Gluteal, hip rotator, and rectus abdominis myofascial trigger points
- Reduced hip mobility and gluteal strength
- Obturator internus palpation reproduced the pain he felt with sexual function
- Severe pelvic floor muscle (PFM) tension at the urogenital triangle
- Pain at the perineal body with palpation
- Impaired PFM length-tension relationship contributing to his inability to contract and lengthen the PFMs
Assessment
I suspected due to Chris’ sedentary lifestyle as a pilot that the constant compression on the PFMs were causing tension and a reduction in blood flow to the area resulting in pelvic pain and pelvic floor muscle dysfunction. The PFMs, more specifically the muscles of the urogenital triangle, attach to the perineal body which can cause perineal pain and I suspected his painful sitting. They are also the muscle group responsible for urinary and sexual function. The severe tension found in these muscles I suspected were contributing to his urinary symptoms, painful sitting, and pain associated with sexual function.

Treatment Plan
Chris’ plan included connective tissue and soft tissue mobilization, and myofascial trigger point release of the external pelvic girdle muscles and pelvic floor muscles to address the dysfunction. It also included neuromuscular reeducation to improve flexibility and coordination of the PFMs, and therapeutic exercise with a home exercise program that included strengthening of the pelvic girdle muscles to support the PFM tension.
Outcomes
At 4 weeks he reported less pain with sexual function and he was feeling more normal when sitting prolonged for flights.
At 8 weeks he was having 85% less pain with sexual function. He was staying consistent with his home exercises even while traveling. He reported that his urgency and frequency continued to act up when consuming caffeine. Caffeine is a diuretic and can cause the body to produce more urine. We discussed how he could still have that cup of coffee while staying hydrated to help the urgency and frequency. He progressed with his gluteal and core strengthening exercises to help support his PFM tension.
By 12 weeks of pelvic floor physical and occupational therapy he was able to return to his regular exercise routine. Abdominal exercises in yoga used to flare him up, however he was able to return to yoga and participate in all poses without pain or symptoms. His primary goal that he achieved was that he was able to sit for flights without symptoms and he felt normal. The pain with sexual function had reduced to occasional minimal tightness afterwards. He reported feeling confident he could manage any flare ups in the future because of the tools and exercises that he had learned in PFPT at PHRC.
Conclusion
Pelvic pain can greatly disrupt our daily life, making it challenging to go about our routines, hobbies, and work. With pelvic floor physical and occupational therapy effective relief can be achieved by improving muscle function, reducing tension, and restoring mobility. Through targeted treatment and a personalized plan at PHRC, our male pelvic patients can experience lasting relief, return to the activities they love, ultimately reclaiming their health and well-being.
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
tags: Chronic Pelvic Pain treated, irritable bowel syndrome, chronic pain, chronic pelvic pain diagnosed, physical and occupational therapy, pain relief, pelvic organs, treat chronic pelvic pain, painful bladder syndrome, interstitial cystitis, pelvic floor dysfunction, chronic pain syndrome, pelvic exam, persistent pain