By Jandra Mueller, DPT, PHRC Encinitas & Guest Author Julie Baron, DPT, CSCS, PCES
Having been a pelvic floor physical and occupational therapists for over twelve years, I can count on one hand the amount of times I have seen this diagnosis; yet, some sources say it is the second leading cause of chronic pelvic pain. Of the patients I have seen with this diagnosis, all of them were diagnosed accidentally while undergoing treatment for a different disorder.
Understanding Pelvic Venous Disorders
This year I had the incredible opportunity of traveling to Spain where some of the top specialists in sexual medicine got together to update guidelines on various topics concerning sexual medicine. I was on a committee reviewing a specific diagnosis – persistent genital arousal disorder/genito pelvic dysesthesia (PGAD/GPD) and I was one of two physical and occupational therapistss in attendance. With this particular diagnosis, there is so much we still do not know, and a region based assessment has been developed in better diagnosing and determining appropriate treatments for individuals who suffer from this condition. The region I was assigned was Region two, the pelvic floor, pudendal nerve, and vascular contributions. At this point, the role of the pelvic floor and pudendal nerve had been pretty thoroughly reviewed, but the vascular component was something I had wanted to take a deep dive into.
Finding this information was not so easy it turns out. Luckily, I was introduced to an online course called “A Comprehensive Look at Pelvic Venous Disorders” by Julie Baron, DPT, CSCS, PCES which was recently adopted by APTA. After taking her course, I connected with her and she has been a true gem in breaking down this complex condition. Julie is the Director of the Pelvic Health and Performance Center at MTI physical and occupational therapy in Washington State, and a genuine expert in this field.
Needless to say, I was very intrigued, and I want to share what I’ve learned in this process with you all.
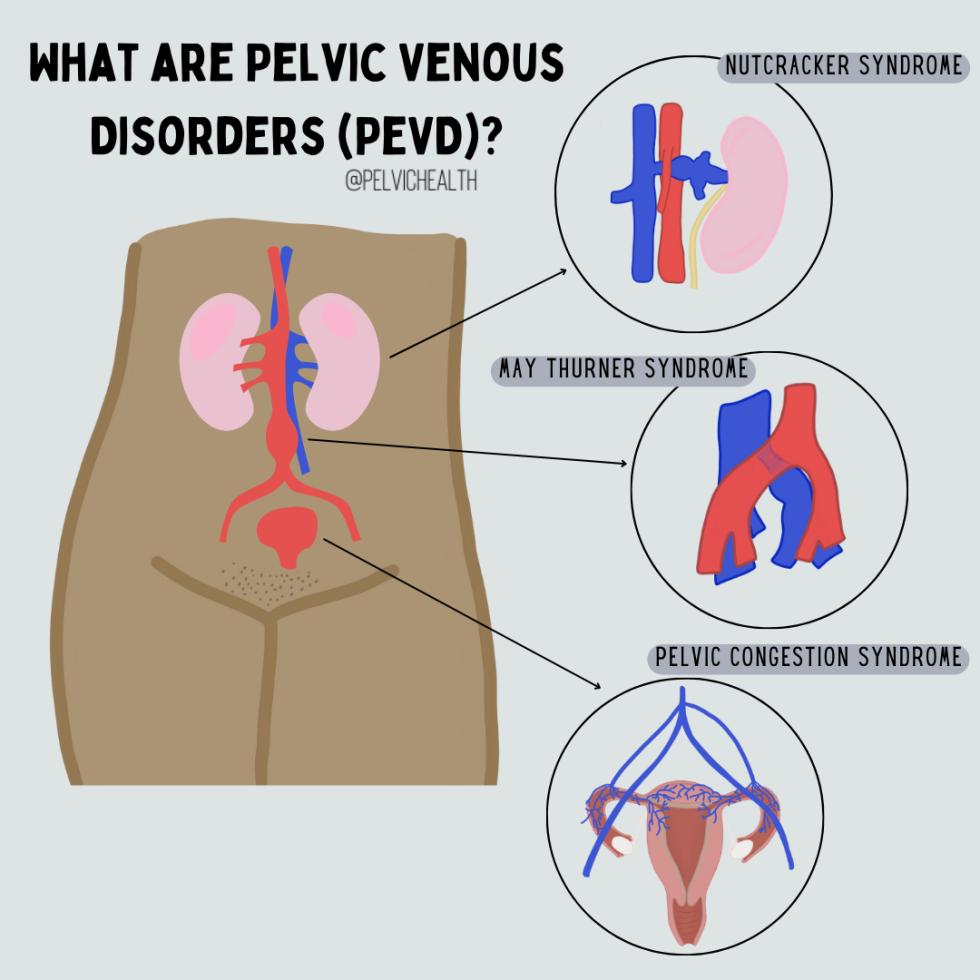
What is Pelvic Venous Disorders PeVD?
Pelvic venous disorders (PeVD) are a group of disorders referred to as “Pelvic Congestion Syndrome (PCS),” “Nutcracker Syndrome (NCS)” or “May-Thurner Syndrome (MTS).” PeVD is an encompassing term that includes both venous obstruction disorders (NCS & MTS) and venous reflux disorders (PCS). Changes in terminology have been a big step forward for those suffering from these conditions in order to provide comprehensive care from diagnosis through treatment. Previously, individuals suffering from these conditions have encountered misdiagnoses and/or incomplete treatment due to the lack of knowledge surrounding these conditions. Clinicians and researchers have now agreed upon PeVD as it encourages a more thorough diagnostic workup, covering both obstructive and reflux disorders.
When it comes to chronic pelvic pain, there can be so much to learn. Read along as we discuss pelvic venous disorders, the pelvic pain associated with it, along with symptoms, treatments and relevant information about pelvic congestion syndrome (aka pelvic venous disorders).

Symptoms and Prevalence
PeVD manifests through a spectrum of symptoms affecting the abdomen, pelvis, and legs. One of the most common symptoms, though not commonly recognized by many providers, is chronic pelvic pain lasting more than six months. This pain is typically described as a dull ache, heaviness, or pain in the lower abdomen or pelvis that worsens with prolonged standing, activity, following intercourse or arousal, and the Valsalva maneuver; and improves when lying down or assuming inverted positions. Studies have indicated that 15-30% of people assigned female at birth (AFAB) aged 18-50 may experience PeVD, although only about 40% are referred to specialists for treatment. PeVD is often associated with multiparity, high estrogen levels, genetics, and hypermobility spectrum disorders, although its exact causes remain largely unknown.

While these individuals are the most likely, we do know that young, premenopausal people who have not had children, or those who are in menopause are not exempt from this condition.
Diagnostic Approaches
Getting a diagnosis can be quite challenging. In an ideal situation, your symptoms would be recognized by a provider, who will then refer you to a provider for further workup, usually a vascular doctor or interventional radiologist.
Diagnosis of PeVD involves multiple imaging techniques and clinical assessments. The first-line screening method is ultrasound (US). Ideally, a transabdominal duplex US which can look at different regions to provide a comprehensive evaluation of each system.
Transvaginal Ultrasound (TVU)
More effective in ruling out other gynecological problems.
Transabdominal Ultrasound
Allows visualization of all the vessels potentially involved.

What Happens If I need more testing?
In cases where ultrasound results are inconclusive or more extensive imaging is needed, computed tomography (CT) and magnetic resonance imaging (MRI) may be recommended but do have their disadvantages; however, venography is the gold standard for diagnosis. Despite venography being the gold standard, it is often reserved for when non-invasive imaging is inconclusive and interventional therapy is being planned.
While many providers will still utilize laparoscopy as a last resort for diagnosing chronic pelvic pain, they may miss up to 80-90% of PeVD cases due to positional vein compression and the use of carbon dioxide during the procedure.
Treatment Options
The primary treatment for PeVD involves endovascular therapies including sclerotherapy, embolization and/or stenting. Which treatment is dependent upon all of what is going on may include one or more of the above treatments. Studies have shown that embolization has a very high technical success rate, close to 100%, with significant symptom improvement in more than 66% of patients. However, recurrence rates can vary widely, ranging from 7-93%, likely due to a lack of standardization or accreditation in this area.

Before the advent of endovascular treatments, reducing estrogen levels through medications like medroxyprogesterone or GnRH agonists was the first-line therapy. Surgical options included hysterectomy and laparoscopic ovarian vein ligation, both demonstrating various levels of symptom relief, but ultimately not addressing the root cause of the issue! Despite the reported “effectiveness” of these treatments, studies often utilized non-standardized questionnaires, making it difficult to fully capture the impact on patients’ quality of life.
What role does the pelvic floor play in PeVD?
Generally, pain conditions are associated with high-tone or overactive pelvic floor muscles, which are often painful when palpated. The impact on the body extends beyond just the muscles in the pelvis, the pelvis in general, along with all the muscles surrounding the pelvis, may be stuck in patterns that do not serve us well, further exacerbating symptoms. That is where pelvic floor physical and occupational therapy comes into play! While we cannot fix the actual veins, we can optimize the body to reduce symptoms and provide an environment that encourages blood flow. Ultimately, treating PeVD requires a team.

Multidisciplinary Treatment Approaches – What To Do If You Suspect PeVD?
Find a Specialist!
Because there is no standardization of treatment or accreditation process for approaching PeVD, it makes it difficult to find the right provider. Both vascular docs and interventional radiologists can treat this condition, they need to undergo specialized training. Just because they may be able to stent or embolize elsewhere in the body, does not mean they are qualified to treat PeVD.
Similarly, pelvic floor physical and occupational therapistss may not be aware of this condition either. Julie has been working hard to create a directory so that patients can find the help they need. Hopefully this will be accessible in the near future, but for now, she has created a list of questions that can help you find someone that can help.

Questions to ask your provider:
Do you work with patients who have PeVD?
What % of your caseload is made up of people with PeVD?
What is your evaluation process and what imaging do you recommend?
What are your preferred treatment strategies for people with PeVD?
What are your clinical outcomes like post-surgery/post-treatment?
Do you have a physical and occupational therapists you can recommend before/after treatment?
Don’t be surprised if the answer is “it depends,” because the presentation and symptoms vary between patients, it truly may depend how they approach your care. What you’re looking for is a provider who is going to consider your unique case, provide a full evaluation including imaging (all four veins), and then discuss treatment options which should involve one of the following or a combination of the following: embolization, stenting, and/or sclerotherapy.
Closing Thoughts
PeVD is a complex condition that necessitates a comprehensive and multidisciplinary diagnostic and treatment approach. While advancements in imaging techniques and endovascular treatments have significantly improved the management of PeVD, there remains a need for standardized protocols and large-scale clinical trials to further enhance patient outcomes. Understanding the interplay between PeVD and associated conditions such as pelvic floor dysfunction, is crucial in providing holistic care to affected individuals.
Drop your questions in the comments for our follow up Q&A blog about pelvic venous disorders/chronic pelvic pain!
Questions and Answers
Q: Is PeVD the same thing as pelvic congestion syndrome?
A: Yes. pelvic venous disorders (PeVD) is also known as pelvic congestion syndrome (PCS).
Q: Could you talk about pelvic venous insufficiency next?
A: We can certainly to a follow up to this blog to go in depth about more questions and side bars within the blog! Feel free to leave more comments for us to be included.
Q: If I have chronic pelvic pain, should I be concerned about developing this?
A: Managing your pelvic pain with a multidisciplinary team of providers would be a great way in tracking your health in order to prevent it from developing further. Each chronic pelvic pain case is different from another. If you are concerned about pelvic congestion syndrome, we suggest speaking to your provider about it!
______________________________________________________________________________________________________________________________________
Resources
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Now Scheduling in Ohio!
Did you know we opened our 11th location in Columbus, OH? Call (510) 922-9836 to book!
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Want more?
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok