
By Stephanie Prendergast, PHRC Cofounder
What is Vulvodynia? Is it a symptom, a disease, or a syndrome? What does the term ‘Vuvlodynia’ mean to people with vulvar pain, pelvic pain specialists, medical professionals, and the community in general?
In a previous blog post I wrote about how in the pelvic pain world, diagnosis does not dictate treatment. Many pelvic pain diagnoses simply describe the location of the pain, but they do not tell us how the problem developed, what is causing it, or how to treat it. “Vulvodynia” means pain in the vulva, and I consider that to be a symptom.
On April 8th and 9th, I was honored to be one of 28 vulvoaginal experts invited to participate in the International Consensus Conference on Vulvovaginal Pain (Vulvodynia) Nomenclature (click here for the entire list of participants).The event was organized by Dr. Andrew Goldstein and ISSWSH. The motivation for a consensus meeting originated because “there is an unmet medical need for a comprehensive, evidence-based set of vulvovaginal pain diagnoses that can be easily utilized by both expert and non-expert healthcare providers to establish diagnoses in their patients and to guide treatment.”
{kind=link}
The Mission of the group was to develop evidence-based consensus among experts, experienced in the diagnosis, evaluation, treatment and/or research in vulvovaginal pain for women, for appropriate nomenclature and definitions of female sexual dysfunctions. These definitions must be applicable across disciplines and useful in both clinical and research settings, and to serve as the basis of ICD codes for women’s sexual health problems.
The conference began with a historical overview of current vulvar pain terminology:
“Vulvodynia has been defined by the International Society for the Study of Vulvovaginal Diseases (ISSVD) as chronic vulvar discomfort, most often described as a burning pain, occurring in the absence of relevant visible findings or a specific, clinically identifiable, neurological disorder,”Patients can be further classified by the anatomical site of the pain (e.g. generalized vulvodynia, hemivulvodynia, clitorodynia) and also by whether pain is provoked or unprovoked.” Chronic is considered longer than 6 months.
The above definition was voted and agreed upon…..in 2003. I began working with people with pelvic pain in 2001, and I can tell you there have been tremendous advances in the management of these disorders. Reading this archaic, horrendous definition left me thinking WTF? How would I feel if I was diagnosed with Vulvodynia, and read online that it is chronic (doomed for life!), absence of relevant visible findings (I suppose it is all in my head and the fact that I am in pain is ‘irrelevant’), and that I would be ‘classified’ based on where my pain is?
I can say for sure that we do have identifiable causes, we do have visible findings, and women with vulvar pain have a treatable condition, NOT an unresolvable medical mystery. I was grateful this conference had been organized, because patients are being thrown under the bus. Tensions were running high as we shifted into the morning lectures on possible physiological causes of vulvar pain:
- Inflammation (David Foster, MD MPH)
- Neuroproliferation (Jacob Borenstein, MD, MPA)
- Hormonal (Andrew Goldstein, MD, FACOF, IF)
- Genetic ( Nina Bohm-Starke MD, PhD)
- Peripheral Neuropathic (Lee Dellon, MD, PhD, FACS)
- Central Neuropathic (Melissa Farmer, PhD)
- Musculoskeletal (me!)
- Psychosocial (Caroline Pukall, PhD, C.Psych)
- Systemic (Deborah Coady, MD)
Listening to the lectures on these 9 evidence-based vulvar pain subsets confirmed why I consider ‘Vulvodynia’ a symptom and not a helpful diagnosis. I used five actual case examples to make this point that more developed nomenclature is necessary to help suffering women get appropriate treatment. The five women I described all have ‘Vulvodynia’.
Leah is 30 years old. Her vulvar pain developed following multiple urinary tract infections that were appropriately treated with antibiotics but unfortunately led to multiple yeast infections. Her treatment plan included manual therapy to treat high-tone pelvic floor muscles and vulvar connective tissue restrictions. Leah also needed to work with a naturopathic doctor to get to the underlying cause of the repetitive infections. Both the musculoskeletal dysfunction, inflammation, and the systemic infections were primary causes of Leah’s vulvar pain.
Michelle is 30 years old. Her vulvar pain developed after she was in a car accident. During the car accident her knees hit the dashboard, causing sacroiliac joint dysfunction. Because of the close relationship between the sacroiliac joint ligaments and the pudendal nerve, she subsequently developed pudendal nerve irritation which in turn caused a high-tone pelvic floor and constant vulvar pain. Because of the pudendal nerve irritation, Michelle could not initially tolerate physical and occupational therapy. I referred her for a pudendal nerve block (peripheral neuropathic treatment), then we resumed physical and occupational therapy that included manual therapy as well as orthopedic treatment strategies for her sacroiliac joint (musculoskeletal treatment), which was a driving factor in Michelle’s case (but clearly not in Leah’s case above).
Gwen is 49 and a triathlete. Her vulvar pain started two weeks after she started an exercise regime called Crossfit. She noticed the pain when she attempted to have intercourse. This scared her; she did a google search on ‘pain with sex’ and thought she had pudendal neuralgia. I fully expected her to have numerous trigger points and pelvic floor tone issues based on her athletic history. Instead, I discovered that her periods have been irregular and she is in peri-menopause. Upon inspection, her vulvar tissues were thin and lacking estrogen. Her musculoskeletal structures were totally normal. The vulvar pain with intercourse coincided with a change in her exercise routine, but it also coincided with resuming intercourse after a period of inactivity and perimenopause. Her treatment consisted of topical hormonal cream and she did not need physical and occupational therapy.
Michelle, who is 23 years old, always had painful periods and was using oral contraceptives to reduce her painful periods. She began to experience vulvar pain with tampon use, and for two years she experienced vulvar pain with insertion. She then developed a Bartholin’s cyst that was surgically removed. Following this procedure, she felt daily pain at the incision site. Upon physical examination I could feel scar tissue at the surgical incision site and identified other musculoskeletal findings that were likely contributed to her provoked pain. It is plausible that androgen insufficiency from oral contraceptives was a contributing cause to the provoked vulvar pain that developed with insertion and that a neuroma secondary to surgery was contributing to the daily unprovoked pain. Her treatment involved cessation of the birth control pill, topical and systemic hormonal therapy, surgical excision of the neuroma, and physical and occupational therapy. Her case was hormonal, genetic, peripheral neuropathic, and musculoskeletal.
Barb is 53 and the mother of two children, ages 25 and 27, delivered vaginally. She underwent a complete hysterectomy and anterior vaginal wall repair for uterine and bladder prolapse. Mesh was used in this repair. Following surgery, Barb developed severe and debilitating vulvar pain. Her pain was caused by peripheral nerve irritation from the mesh and it eventually was removed. Following the removal of the mesh she underwent pharmacologic therapy for CNS hypersensitivity, pudendal nerve blocks, and physical and occupational therapy, which resulted in resolution of her symptoms.
All five women have ‘Vulvodynia’ for different reasons. And we do know what they are.
Following the physiology lectures, we heard presentations on physical examination findings and tests for women with vulvar pain. These include visual and palpation examination of the vestibule, examination of the pelvic floor muscles, histopathology, laboratory testing and psychometric evaluation.
Next, we were broken into 5 small subgroups with four objectives in mind:
- Develop, through expert consensus, nomenclature describing vulvovaginal pain (vulvodynia) and subgroups of vulvovaginal pain.
- Utilize the nomenclature developed to establish diagnostic criteria for vulvodynia and its subgroups.
- Utilize the nomenclature developed to establish evidence-based treatment guidelines.
- Utilize the nomenclature developed to develop suggested areas of future research.
On day two, one leader from each breakout group presented their group’s suggested nomenclature; there were five options to chose from. 28 of us voted and one group’s option was chosen. We then spent the rest of the day in animated, thoughtful, heated and intense discussions, debating what the evidence does and does not tell us, how nomenclature can support both researchers and clinicians, and how to support nonexpert and expert clinicians and most importantly, women suffering from vulvar pain.
At the 13th hour we did reach a consensus!
- We agreed to change the title of Vulvar pain classification from ‘Chronic Vulvodynia’ to ‘Persistent Vulvar Pain’.
- Evidence supports 7 subclassifications of vulvar pain
- Infectious
- Inflammatory
- Neoplastic
- Neurological
- Trauma
- Iatrogenic
- Hormonal deficiencies
- Vulvar pain can exist without an identifiable cause
- Vulvar pain can be described as localized, provoked, by onset (primary or secondary) or by temporal patterns (intermittent, persistent, constant, immediate, delayed)
- Vulvar pain is associated with certain factors (IMPORTANT: there was not enough evidence to support cause or effect, we can state we know vulvar pain can exist with the following impairments)
- Neuoproliferation
- Musculoskeletal
- Psychosocial
- Genetic
- Hormonal
- Neurological
- Peripheral neurologic
- Central neurologic
- Comorbid pain syndromes
This classification has the potential for tremendous improvement in clinical care for our suffering patients. I was honored to be part of it and to see how far we have come in 15 years, we just need our nomenclature to show it.
The results of our meeting are currently being written up and submitted to the International Pelvic Pain Society, The International Society for the Study of Vulvovaginal Disease, and The National Vulvodynia Association. We are hoping that these three societies will adopt the new nomenclature and that they will become part of the ICD coding.
Readers we want to hear from you! If you have any questions please do not hesitate to leave them in the comment section below.
And if you haven’t already, SUBSCRIBE to this blog (up top, to the right, under my photo!), so you can get weekly updates in your inbox, and follow us on Facebook and Twitter where the conversation on pelvic health is ongoing.
All my best,
Stephanie Prendergast, MPT
 Stephanie grew up in South Jersey. She received her bachelor’s degree in exercise physiology from Rutgers University and her master’s in physical and occupational therapy at the Medical College of Pennsylvania and Hahnemann University in Philadelphia. For balance, Steph turns to yoga, music, and her calm and loving King Charles Cavalier Spaniel, Abbie (Abbie is a daily fixture at PHRC Los Angeles). For adventure, she gets her fix from scuba diving and global travel. One of her most recent adventures took her to China.
Stephanie grew up in South Jersey. She received her bachelor’s degree in exercise physiology from Rutgers University and her master’s in physical and occupational therapy at the Medical College of Pennsylvania and Hahnemann University in Philadelphia. For balance, Steph turns to yoga, music, and her calm and loving King Charles Cavalier Spaniel, Abbie (Abbie is a daily fixture at PHRC Los Angeles). For adventure, she gets her fix from scuba diving and global travel. One of her most recent adventures took her to China.
FAQ
What are pelvic floor muscles?
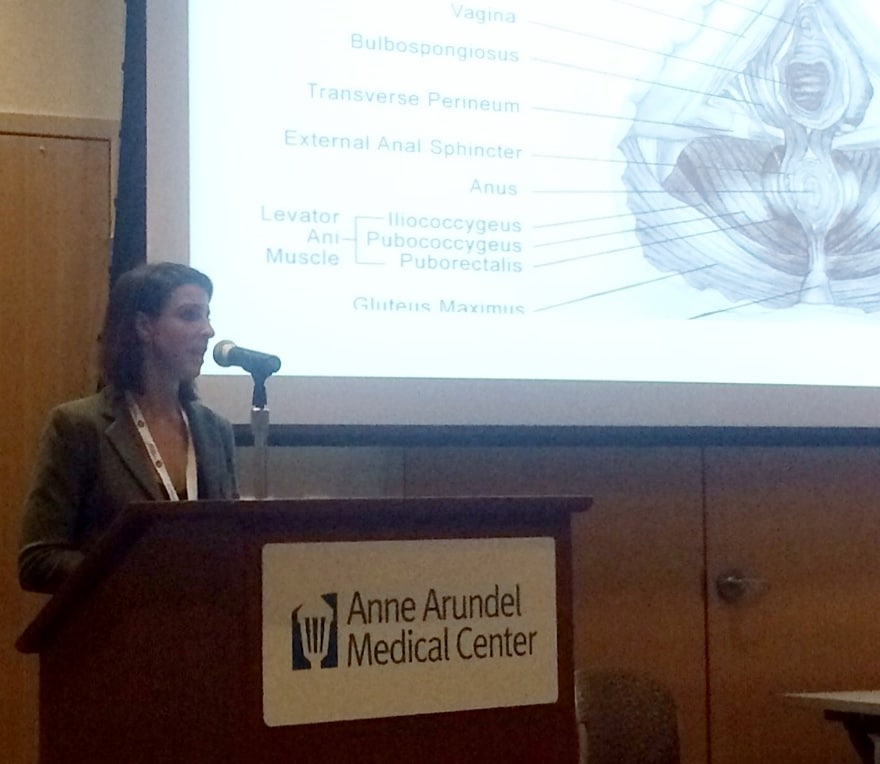
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
Stephanie… Your guys’ work is invaluable!! Reading the information gave me a sense of epiphany as I have been working with lots of women with pelvic pain and realized that the variations from where the pain can arise is significantly larger than I thought!! It’s the central sensitivity associated with lifestyle, where in life a woman is, general health, surgeries, hormones, etc!! I hope your nomenclature does stick and allows all of us including the patient to adopt this info.. So many people in the medical community looks at this as a separate issue and it ‘s not! It’s the whole person! Thank you!!
Hello Teo,
Thank you!
All my best,
Stephanie
Thank you for your work in this area. I completely agree with your comments on how inadequate the diagnosis is and how hopeless it sounds, especially at the time of diagnosis when we start researching the DX. I am so grateful for my PT and for you and others working in this area of PT.
Thank you!
On behalf of all Pelvic Floor & women’s health PTs, we salute you for your siginificant contributions into this ISSVD meeting!
Your blog posts & studies with the rest of PHRC staff continue to educate me. Being a rural Pelvic PT & working alone is not easy but having access to all your blogs, & studies allow me to expand my critical thinking & pathways to approach patient’s clinical presentations in my daily practice. Thank you so much for sharing your expertise thru your blogs here!
Annette,
Thank you so much for your kinds words! We believe in creating and encouraging healthy a dialogue with patients and providers about the ever changing world of pelvic floor dysfunctions. If you have not yet attended our course, “Demystifying Pudendal Neuralgia As a Source of Pelvic Pain: A Physical Therapist’s Approach” you may want to consider it! It provides a wealth of information, training, and resources for therapists and providers.
All my best,
Stephanie
Hi Stephanie,
I have been wanting to catch this course here in the West Coast, are you having one here in our area this year? Hopefully, in Northern California?
Please consider & let me know.
Thank you again for all your contribution in Pelvic PT!!!
Hello Annette,
We will consider it, but our upcoming course will be in Arkansas Sep. 12-15, 2015. Our website will provide more information if your choose to attend.
All my best,
Stephanie
Nicely reviewed! Did anyone attempt to show primacy of one subtype across duration of symptoms or over the lifespan
Very grateful for IPPS’s contributions and your engagement in this critical area.
Thank-you Frank. We are gathering the levels of evidence regarding subtypes this week. Andrew Goldstein is aiming to have the paper completed in time for the ISSD in July.
Stephanie,
Thank you for such a great summary of the consensus meeting. I have been working with vulvodynia patients for a while now. The more I learn about it, the more I realize so little we know about this fascinating complex condition. Thank you so much for your great job done at the IPPS.
Warm regards,
Jose “Tony” Carugno
Thank-you Tony! Come say hi at the IPPS meeting this year in San Diego! http://www.pelvicpain.org
While I appreciate the effort all of you have/are putting into trying to define vulvodynia more accurately, as a patient I’d like to know what this means for me and others who suffer from these symptoms? I have given my doctor a detailed written history of the progression of my symptoms describing location types and qualities of pain. I have been through PT, biopsies and more drug therapies than I can remember, almost 6 years after onset…and I am now at the point where I am suggesting hey-what-about-this-I-saw-on-Reddit therapies to my doctor, instead of her tailoring therapies according to specific possible causations based on my history. It’s frustrating to see news like this when the quality of life of patients isn’t affected. So when will these breakthrough diagnosis refinements mean something real to your patients?
Hello Christine,
We agree that the pace in which new treatment protocols, and knowledge regarding pelvic floor dysfunctions is accepted can be frustrating. However, what we discuss in this blog already “means something very real” to patients. It means we are moving forward in the right direction, and although the larger medical community has yet to fully evolve, much progress continues to be made on a daily basis, more physical therapists are joining our ranks, and the RIGHT treatment is becoming more accessible across the globe. If you are in need of a therapist who can help you, I may be able to recommend a therapist. Where are you located?
Best,
Stephanie
Thank you for your response. I am in Michigan, near Detroit.
Hello Christine,
Below are therapist recommendations in your area:
Justice Jamie PT Dekalb IL (815) 785-5508 Creative Therapeutics
Markett Kristen PT Orland Park IL (708) 671-1971 Flexeon Rehab
Thatcher Judy PT, CFMT Cary IL 8474581722 Sherman Hospital
O’Keefe Maureen PT Evergreen Park IL 6306200232 1 Trans America Plaza Dr
Kirk Brandi PT Homer Glen IL 7083013102 Kirk Center for Healthy Living
Florendo Judith PT Evanston IL 3123378840 Florendo Physical Therapy
Best,
Stephanie
Do you have any PT recommendations in Cleveland, Ohio? I have been tested for many things and have been told my constant feeling of the need to urinate maybe caused by PF dysfunction. It came out of nowhere. No other significant symptoms? I am 54 and healthy. Thank you.
Hello Betsy,
Please use the below link to find a pelvic floor physical therapist in your area.
https://pelvicguru.com/2016/02/13/find-a-pelvic-health-professional/
Regards,
Admin
I have been diagnosed with vulvodynia. Is it possible that this was caused by excessive “fingering”.
This condition started right after I had this sexual affair almost 2 years ago. Did not have sex for over 20 years prior, and my pain started right after this event in 2014. Could my pudendal nerve have been damaged?
Author Stephanie Prendergast says:
It is not likely that your pudendal nerve was damaged, but it is plausible that there were vulvovaginal issues that you were unaware of until this sexual encounter. It makes sense to see a gynecologist that specializes in pelvic pain to identify vulvar atrophy or a dermatologic issue. and possibly a pelvic floor physical therapist.