By Melinda Fontaine, DPT, Walnut Creek

At the 3rd World Congress on Abdominal and Pelvic Pain organized by the International Pelvic Pain Society, Professor Qasim Aziz spoke about Autonomic Dysregulation in Functional Gastrointestinal Disorders. Qasim Aziz, MBBS, FRCP, PhD is Professor of Neurogastroenterology at Barts and The London School of Medicine and Dentistry at Queen Mary, University of London. Professor Aziz taught us how the autonomic nervous system plays a role in chronic pain conditions and functional gastrointestinal disorders. This understanding has led to the use of new treatments that modulate the autonomic nervous system.
The autonomic nervous system is made up of the brain, the parasympathetic and sympathetic nervous systems, and the enteric (gut) nervous system. The autonomic nervous system works without us having to think about it, and helps with things like keeping our heart beating and digesting our food. The parasympathetic nervous system is affectionately called the “rest and digest” system because it is active when we are relaxed and helps with digestion. When you add stress to the equation, big changes occur. Stress can be in any form: deadlines, anxiety, drama, attack on your health, lack of sleep, not enough self care, etc. When stress is applied to the system, the peripheral nervous system releases neurotransmitters which dock on the immune cells and increase the inflammatory immune response through the vagus nerve.
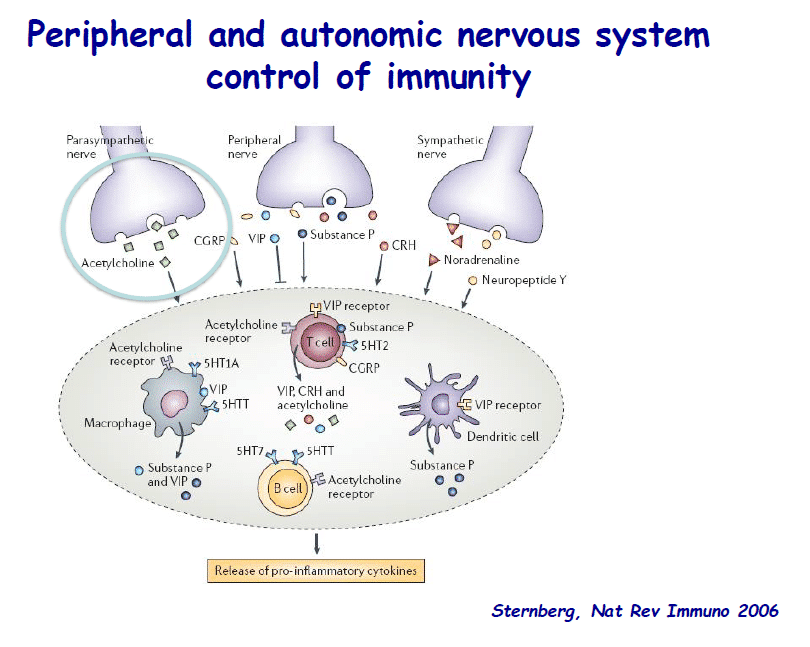
Now if all that sounded like scientific mumbo-jumbo, the important piece to remember is “through the vagus nerve”. The vagus nerve is part of the parasympathetic “rest and digest” nervous system and innervates the heart, lungs, and digestive system.
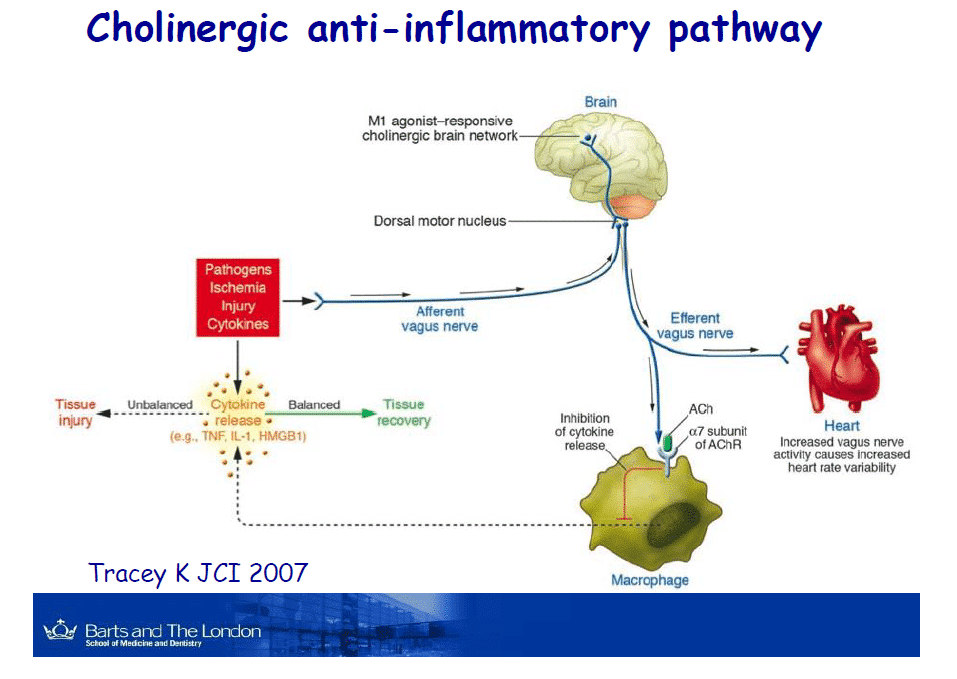
A number of studies have been done on the role of the peripheral nervous system and vagus nerve. Decreased peripheral nervous system/vagus nerve activity has been found in patients with irritable bowel syndrome,1 functional dyspepsia,2 and delayed gastric emptying after meals.3 Could we increase the vagus nerve activity to eliminate these and other symptoms? Possibly! There are three treatments being explored to stimulate the vagus nerve and decrease pain and inflammation.
- Cognitive Behavioral Therapy increased vagus nerve/parasympathetic activity in patients with irritable bowel syndrome over the course of 24 weeks.4
- Deep Breathing increased vagus nerve/parasympathetic activity and decreased pain in the esophagus in response to acid.4
- Vagus Nerve Stimulation improved movement of food through the digestive system,5 reduced abdominal pain,6 and decreased inflammation.7
Cognitive Behavioral Therapy is a common method of psychotherapy and Deep Breathing has been around for ages, but Vagus Nerve Stimulation is new, and I would like to explain it a little here. For more information about how this idea relates to chronic pelvic pain, see Liz’s post about Dr. Chelimsky’s presentation.
Applying electrical current to the vagus nerve through an implantable or external device amplifies the signals sent through the nerve. The devices work by attaching electrodes to the vagus nerve either at the ear or the neck. Not all these devices are available in the United States, and they currently require a doctor’s prescription. These devices have also been studied for use on headaches, seizures, depression, fibromyalgia and chronic pelvic pain.8 These treatment are relatively new and are still being studied, but the research is promising.
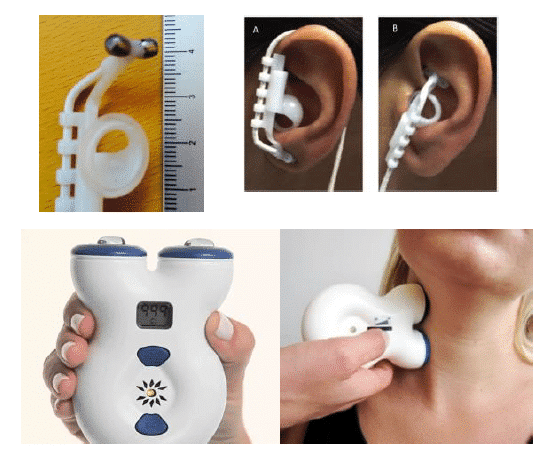
Of course this information made me very excited about this new vagus nerve treatment idea. I want to run right out and get my hands on a stimulator. After some research, I learned that the FDA released the first non-invasive vagus stimulator in 2017, gammaCore. This device applies stimulation at the neck for the acute treatment of pain associated with episodic cluster headache in adult patients. It is available by physician prescription only, and the list price of gammaCore therapy is $575.00 per month.
Thus, for now I will have to use the treatment strategies most available to me. I like to remind patients that pelvic pain is rarely ever caused by one thing, so a multimodal approach that includes physical and occupational therapy is necessary. This research shows us how the parasympathetic nervous system needs to be considered in our treatment approach. I teach patients to breathe deeply during our sessions and encourage them to practice on their own. I use Nicole’s blog about diaphragmatic breathing to teach the technique. Sometimes I encourage patients to seek out psychotherapy, such as cognitive behavioral therapy, as a piece of their treatment. One day, I may also be able to recommend vagal nerve stimulation as part of a complete treatment approach.
We thank Professor Qasim Aziz for a fantastic lecture. Please click here to view his entire lecture.
References:
- Liu Q, et al. Autonomic functioning in irritable bowel syndrome measured by heart rate variability: A meta-analysis. Journal of Digestive Diseases 2013; 14: 638-646
- Dal K, et al. Decreased parasympathetic activity in patients with functional dyspepsia. European Journal of Gastroenterology & Hepatology 2014, 26:748-752
- Guo WJ, et al. Impaired vagal activity to meal in patients with functional dyspepsia and delayed gastric emptying. J Int Med Res 300060517726442. 2017
- Botha C, Farmer A, et al. Preliminary report: modulation of parasympathetic nervous system tone influences oesophageal pain hypersensitivity. GUT 2015, 64:611-7
- Frokjaer JB, et al. Modulation of vagal tone enhances gastroduodenal motility and reduces somatic pain sensitivity. Neurogastroenterol Motil 2016; 28, 592-598
- Kovacic et al. Neurostimulation for abdominal pain-related functional gastrointestinal disorders in adolescents: a randomised, double-blind, sham-controlled trial. Lancet Gastroenterol Hepatol 2017; 2: 727-737
- Beckers AB, et al. Gastrointestinal disorders in joint hypermobility syndrome/Ehlers-Danlos syndrome hypermobility type: a review for the gastroenterologist. Neurogastroenterol Motil 2017; 29: doi: 10.1111/nmo.13013. Epub 2017 Jan 13
- Chakravarthy, et al. Review of vagal nerve stimulation in use of chronic pain management. Current Pain and Headache Reports Journal 2015; 19:54
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.