
I remember coming of age as a hormonal teen- before the days of google (believe it), hearing whispers about “orgasms”. It was like I went home for summer break with all of my childhood intact and when I came back to school in the fall, my peers were suddenly obsessed. I was bombarded with comments (from both sexes) of orgasms and boners and what “your O face” looked like. I remember the secretive giggles while referring to the Herbal Essences commercials and that scene with Meg Ryan in When Harry Met Sally. Or that time in Friends when Monica drew up a map of erotic zones for Chandler (and seemed to orgasm herself while saying the number 7). One of my friends even told me that 8 sneezes was equal to 1 orgasm…I anxiously awaited allergy season just to see if I could experience one of these orgasms by perfectly timing my pollen intake with my sneeze pattern to see if I could nail 8 in a row, and thus reach ORGASM (never, happened by the way).
I was certainly a late bloomer. I was still watching cartoons while others were getting into MTV. I didn’t have any older siblings, my friends were all my age or younger. But seriously, among all of the Cosmo articles with the tips, tricks, and advice about how to make orgasms better- I just had two questions; what are these glorious, yet elusive things? And why are there so many different definitions?
In the Clinical Psychology Review there are 26 different definitions listed for orgasm. Urban dictionary, listed 122 definitions! Here is one of my favorites: “Repetitive ‘Happy Moans’ indicating you have reached the peak of pleasure.” And they used it in a sentence: “Oh! Yes! That’s it! Ah! I’m having an orgasm!” (I even found one definition about the sneezes.) So, in the this week’s blog post I will attempt to give my best explanation of an orgasm. I realize that orgasms can be a combined experience of mental, physical, spiritual, and emotional components. But, since I am a pelvic floor physical and occupational therapists and an expert in the musculoskeletal system, I will focus on the physical aspects of an orgasm.
Before I get too clinical let’s talk about the anatomy. Some of you may remember Rachel’s blogs on penis and vulvar anatomy, which I highly suggest reading at some point. But today, I want to look a little bit closer at what as known as the urogenital diaphragm, the clitoris, and the Gräfenberg “G” spot.
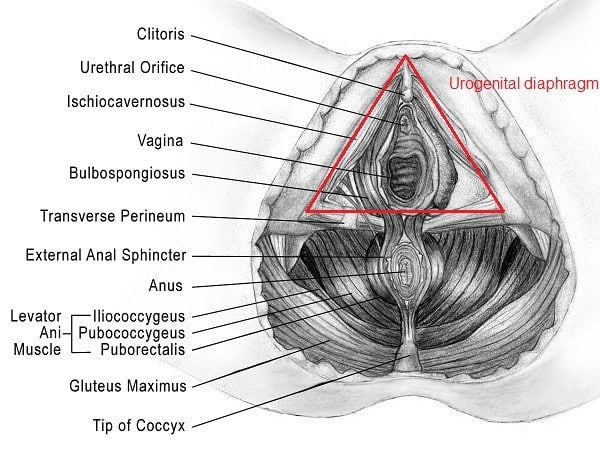
The urogenital diaphragm aka urogenital triangle are the most superficial muscles of the pelvic floor, comprised of the bulbospongiosus, ischiocavernosus, transverse perineum and external anal sphincter. These are the most important muscles during arousal and orgasm.
The clitoris is located above the urethra at the intersection of the labia minora and extends vaginally to a point behind the pubic bone. The clitoris comes from the same cells that form the penis in a male.
The G-spot is typically described as being located 2-3 inches inside the anterior vaginal canal near the intersection of the urethra and bladder and may be of the same cells that go on to become the prostate in men. The G-spot is somewhat controversial between experts in the field because, though it has been studied since the 1940s, scientists have neither been able to prove its location nor its existence in women.
Also, the majority of women report that they need clitoral stimulation in order to orgasm, however this is totally variable from person to person. Research suggests that it is pretty common for women to report that they do not orgasm with penetrative sex alone.
Ok now let’s get to some of the more ahem…dry stuff regarding orgasm:
There are 4 phases of the sexual response cycle:
- excitement/arousal: in this phase the bulbospongiosus, ischiocavernosus, and pubococcygeus contract in order hold blood in the erectile tissues. In men this will present as an erection of the penis and in women there will be swelling of the clitoris and labia minora.
- plateau: pelvic floor muscle tension increases and prepares for orgasm
- orgasm: for both men and women an orgasm will produce rapid muscle contractions of primarily the superficial pelvic floor muscles (bulbospongiosus, ischiocavernosus, and pubococcygeus). Masters and Johnson found through direct observation that a male orgasm lasts approximately 10 to 30 seconds while a female orgasm lasts about 13 to 51 seconds. Interestingly, the interval of contraction is exactly the same for men and women-once every 0.8 seconds. So, you do the math-it’s a lot.
- resolution: phase in which further sexual stimulation does not produce excitement; varies between male and females
There are obvious differences between male and female orgasms, the most obvious being that male orgasms often culminate in ejaculation; however, there are some sex experts that say that men can learn to separate orgasm and ejaculation. Females can experience ejaculation as well, but it is not as common. Most of the research on this topic is incredibly old and outdated but just last month a study came out of France that explained the some of the mystery of the female ejaculation-turns out that it’s mostly urine coming out of the urethra….thanks France!
Because the superficial pelvic floor muscles are integral to achieving an orgasm, it is important that are functioning well. But what about when these muscles aren’t working as best they can? Here are some examples of issues we come across at PHRC:
- Pelvic/abdominal pain with arousal, orgasm, or afterward
- Sudden or gradual decrease in intensity and/or increased difficulty in achieving orgasm, or possibly aorgasmia; men may also describe decreased force of ejaculate
- Some of us have never been able to orgasm also called aorgasmic
- Persistent genital arousal disorder (PGAD): this is a complex issue that physical and occupational therapy can be very helpful in treating. Please click on the link to read Stephanie’s blog for more information
- Some people will report that they may have “over-masturbated”. While on the topic of orgasms, we should clarify this point. If pain/symptoms are occuring after masturbation and/or orgasm, it is logical that the two seem linked. However, it is not uncommon for the underlying problem to be due to tight pelvic floor muscles rather than masturbation itself.
All of the above issues can be caused by hypertonic pelvic floor muscles and potential trigger points. Think about it, if we need those superficial pelvic floor muscles to maximally contract and maximally relax once every 0.8 seconds for 10 to 51 seconds, that’s a big deal for those muscles. It’s like a major workout; and if they are already in a tightened state then getting them to further tighten, or relax for that matter, is going to be a problem. People with tight pelvic floor muscles often notice difficulty achieving orgasm or diminished orgasm intensity. This change often precedes the appearance of pelvic pain.
If you are experiencing any of the above symptoms consult with your physician and a pelvic floor physical and occupational therapists to address potential issues. All of the issues mentioned in this blog are highly treatable with PT intervention. If you need some help finding a pelvic floor specialist in your area, check out some previous posts on this matter here and here.
*Public service announcement: Can everyone please stop listening to Cosmo when they tell us to do Kegels for improved orgasm? If we are having issues, it is often because these muscles are too tight and trying to strengthen them only causes risk of more problems.*
Ok let me get off of my soap box now. My hope is that after you have read this blog that you will never try to get 8 sneezes in a row just so you can experience a “pseudo-orgasm”. No one experiences orgasms in exactly the same way. And it is because of this inherent variety that orgasms can be hard to explain. But I do know one thing-orgasms are important not only for our mental, emotional, and relationship health but for our pelvic floor muscles too! It is important to understand the anatomy involved and be able to recognize when something is not quite right and seek help.
Readers we want to hear from you! Do you have an orgasm or anatomy question? Please share in the comments section below!
And if you haven’t already, subscribe and follow us on Facebook and Twitter where the conversation on pelvic health is ongoing!
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
I am wondering if it is wrong to be contracting the pelvic floor (intentionally) up to and right before orgasm? I seem to do this without thinking about it. I am being treated for hypertonus of my PF and pain with sex. Thank you!
Author Allison Romero says:
“There is no need to be intentionally contracting your pelvic floor muscles pre-orgasm and since you are currently being treated for pelvic floor muscle hypertonicity, this is an issue that I would discuss with a pelvic physical therapist.”
It happens to me too! I realize and relax…I dont have any condition though and its VERY annoying. I’ve noticed my orgasms are better when I’m completely relaxed its almost if my body is trying to force it. Sucks!
How can i go about getting treatment
Hi Crystal,
Please use the link below to find a pelvic floor physical therapist.
https://pelvicguru.com/2016/02/13/find-a-pelvic-health-professional/
Thanks,
Admin
Hi. Thanks for posting such an interesting and illuminating article. My girlfriend told me to look up “pelvic orgasms” as I’ve never heard of them before. I’ve rarely experienced a woman having several orgasms before but my girlfriend and i seem to be a perfect “fit”. The last time we were together she had 7 orgasms over a 3 hour period. She insists they’re come from further inside as I’m stimulating her g spot. With her, I’m experiencing the best sex of my life!
Hello, I am in a workshop with a group of woman with the focus being pelvic floor health. I’m a bit frustrated because, once again, no one wants to talk about how expressing our sexual selves- having an orgasm and the variety of orgasms we experience, do tie into pelvic floor health. With so many muscles affected by having one orgasm and/or the amount of orgasms a woman can have during one sexual encounter, why is this? Wouldn’t this be one of the best things you could do to exercise/tighten and relax the over tightened pelvic floor?
And yes, no more articles implying your vaginas not tight enough, or “not enough” in the matter! Let’s fully educate to empower every woman!
Excellent article. I definitely love this site. Stick with it!