
I recently had the opportunity to get together with a group of moms through the Holistic Moms Network (HMN) in Fremont, CA. I had put together a talk on what I thought were the most common issues moms of any age might be facing, but I wanted to spend some time asking them what they felt they needed more information about, specifically.
The answer was a resounding question, “How, exactly, am I supposed to do a kegel?”
This answer was not surprising to me. Most women are instructed by their obstetrician (OB) to ‘do your Kegels’ without much direction. This is because an OB’s focus is to keep moms and babies safe, not to teach women how to properly do a kegel. Unfortunately, because musculoskeletal questions associated with pregnancy arise, OBs are put in a position to provide information that lies outside their area of expertise. This is where pelvic floor physical and occupational therapistss can step in and help out.
The problem with just telling someone to ‘do your Kegels” is that, according to recent research, 51% of women could not perform a Kegel properly with verbal cueing alone. And 25% of the women in the study were actually performing the attempted-Kegel in a manner that could promote incontinence and pelvic organ prolapse – the very issues kegels are suppose to help! Kegel confusion has been confirmed through my own clinical experience and conversations with new moms. Most women reading this are probably nodding their heads, yes!
In order for readers to get the full picture of how to Kegel, let’s start with the anatomy:
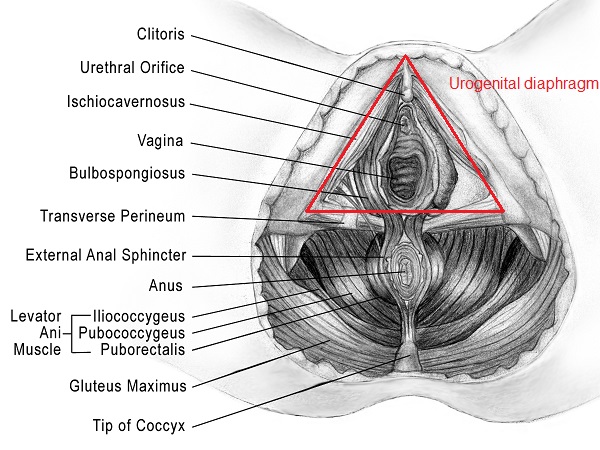
There are two layers of pelvic floor muscles.
The most superficial (closest to the skin) are known as the urogenital diaphragm. These are the muscles that are primarily responsible for helping to close the urethra and anus so that we don’t leak urine/gas/stool when we don’t want to. i.e. laughing, coughing, sneezing, or jumping on the trampoline. When performing a kegel properly you may be able to bias these muscles by concentrating on closing the urethra or anus, and the vaginal opening.
The deeper layer of muscles (closer to the organs) are called the levator ani. These muscles are largely responsible for supporting our pelvis, bladder, uterus and rectum throughout our lifetimes as the forces of gravity, childbearing/rearing, respiratory issues, constipation weigh us down.
Here is a good video of the pelvic floor anatomy and if you haven’t yet become familiar with your vulva read Rachel’s blog.
The basic idea to keep in mind when trying to perform a pelvic floor muscle contraction (kegel) is to squeeze the urethra/vagina/anus closed and lift up. It is an “in and up” motion. When I am palpating someone’s pelvic floor muscles to assess for strength-I am looking for the muscles to squeeze my finger and gently pull it up (toward the head). It is the exact thing that we do if we stop our urine mid-stream. This is not something to get in the habit of doing during urination, due to the risk of urinary tract infections, however it is ok to try one time if it can help you isolate the correct muscles.
Over the past several years at PHRC, I’ve discovered clever cues to help patients find and contract their pelvic floor muscles. Here is my list, but I am sure that there any many other tips/tricks out there. Please share yours in the comments section:
-pull your pubic bone and tailbone together
-bring your sits bones together
-stop the flow of urine
-wink the anus
-nod the clitoris
-pull in like you are putting on a tight pair of jeans
-sit on a chair and pull your perineum up and away from the surface
-think of the muscles as an elevator and “lift” up towards your head
-pull the underwear in
-hold back gas
-like you’re holding a tampon in
If you still feel lost you can try inserting a finger into the vagina or anus and actually FEEL the muscles. C’mon just do it.
You can also try curling your toes while attempting to kegel. (Check out this picture of the homunculus to see how closely related the pelvic floor muscles and feet are.) Also, stay tuned for an upcoming blog on toe curling orgasms!
{kind=link}
If you have made it this far and are still shaking your head in confusion/frustration here’s what you can do:
There are many different products out there that claim to be pelvic floor strengtheners. I strongly recommend checking with a physical and occupational therapists before choosing one, so you get the one that’s right for you. One tool that I have found to be pretty effective and harmless is this pelvic floor educator from Current Medical Technologies. It works like this: you insert it into the vaginal canal and if you are doing a kegel correctly, it gives you visual confirmation.
At PHRC we will sometimes use biofeedback or neuromuscular electrical stimulation (NMES) to help find and isolate these muscles. Biofeedback works by projecting the electrical signals from your pelvic floor muscles on to a screen so that you can see when you are contracting properly. NMES works by supplying electrical signals directly to the muscles making them contract.
Kegels alone are rarely a solution for overall musculoskeletal health but rather one component of an individualized exercise regime for new moms. It is important to learn to do them properly if they are part of your fitness regime (Read here for more info on postpartum rehab). However, not everyone needs to be doing a kegels on a regular basis. In fact, for some people it might even cause dysfunction. Read here to learn why kegels are not right for all of us.
Hopefully this post validates why you might feel confused about how to perform a Kegel, they are definitely an acquired skill! When in doubt, consult with a pelvic floor physical and occupational therapists. They can provide you with an individualized program that is right for you and ensure you know how to do each exercise right. To find a pelvic floor PT: click here.
*Men: I haven’t forgotten about you. Because we are focusing on what mom’s want to hear about I did not talk about the male pelvic floor. But FYI kegels can be really important for you too! Check out these past blog posts for relevant info: here and here.
Readers we want to hear from you! Are you confused about kegels? Please share in the comments section below!
And if you haven’t already, SUBSCRIBE to this blog (up top, to the right, under Stephanie’s photo!), so you can get weekly updates in your inbox, and follow us on Facebook and Twitter where the conversation on pelvic health is ongoing!
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
Great article, but important to note that Kegels are not for everyone (i.e.) patients with tight pelvic floor or pudendal neuralgia.
Hello Anonymous,
Yes, kegels are not for everyone. We discuss that here:
https://pelvicpainrehab.com/pelvic-pain/507/why-kegels-are-bad-for-your-pelvic-floor/
Regards,
Allison
Hey Allison!
Really liked the cues you gave for identifying the right muscles.
I have a question though:
Do kegels lead to tightening of the pelvic floor muscles? Is that why they are important postpartum?
Are there any different kind of kegels or another exercise to prepare the pelvic floor for birth?
Thanks
Parminder
Hi Parminder,
Kegels are prescribed for patients with truly weak pelvic muscles in order to increase strength, and coordination. However, they are not always recommended for postpartum patients since not all new moms actually have weak muscles. Kegels can be important for prenatal care, but every patient is different. We offer specialized prenatal treatment plans for patients that are designed to help with other common issues that may arise such as pelvic girdle pain, and incontinence. I encourage you to consult with a local PF therapist for more information.
All my best,
Allison
What about kegels for men with chronic pelvic pain?
Hello Wayne,
Please read our blog for more information:
https://pelvicpainrehab.com/male-pelvic-pain/2322/men-kegels/
Regards,
Allison
Thank you for the insight on kegels. I have IC and my PT has asked me to do reverse kegels. I’m unclear about how to do them. Any suggestions?
Hello Klyttle,
It is best to communicate any questions or concerns to your therapist. He or she has already evaluated you, and can provide specific advice for you.
All my best,
Allison