By: Jandra Mueller, DPT, MS, PHRC Encinitas
In our second post of our series covering the Third World Congress on Abdominal and Pelvic Pain, I will cover the lecture titled Endometriosis-associated pain, why should we consider the central nervous system? If you missed our first post, click here.

This year at the annual meeting of the International Pelvic Pain Society (IPPS) and the 3rd World Congress on Abdominal and Pelvic Pain (WCAPP), Endometriosis expert Dr. Katy Vincent spoke about why we should not only look at endometrial lesions alone in pain generation (a purely peripheral model), the evidence of central changes in association with endometriosis, and to consider the comorbidities of endometriosis and how it changes clinical practice. In this blog, I will do my best to summarize the complex information from her lecture and help our patients understand what this information mean for them.
What is Endometriosis?
Endometriosis is a disease in which cells similar to the lining of the uterus (endometrium) are found outside of the uterus. More specifically, it occurs when endometrial glands and stroma are found in locations other than the lining of the uterus. It affects 176 million women worldwide, with a percentage ranging from 7-15% of women. The symptoms of endometriosis can include pelvic pain, lower back pain, or painful intercourse, heavy or irregular periods, infertility, GI symptoms such as constipation, bloating, diarrhea, painful bowel movements, urinary symptoms including urinary frequency, urgency, and/or painful voiding, as well as fatigue and general malaise.1 For more information on endometriosis click here.
Traditionally it was thought that endometrial lesions cause inflammation, which compress nerves and cause pain 2. Surgery was thought to remove the lesions and should therefore decrease pain. Dr. Vincent presented four images and asked, who has the most pain?
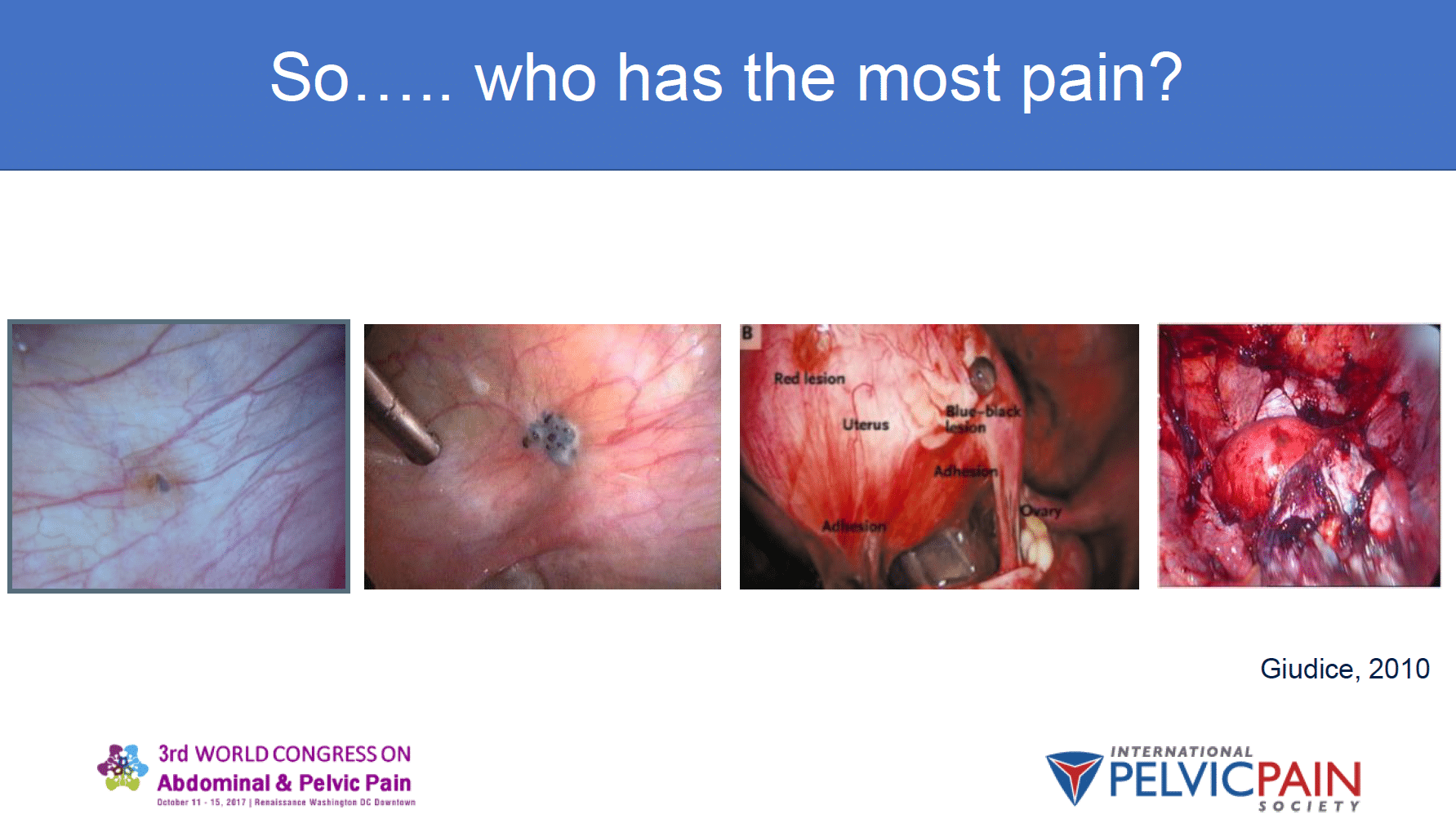
There wasn’t an exact answer, but the point being was that women who experience a lot of pain may have very small lesions whereas women who do not experience pain may have extensive lesions.
As research advanced it became clear there is a minimal relationship between the location of the lesions or the severity of the disease and the amount of symptoms, or severity of symptoms a woman experiences. 3
However, Dr. Vincent does make the distinction that there are associations between the subtypes of endometriosis that do correlate with symptoms. For example, deep infiltrating endometriosis (DIE) is consistently associated with chronic pelvic pain (CPP), but the presence of endometriomas (which is a severe form of the disease) is not associated with the severity of dysmenorrhea (painful periods).4
What does this mean? Take home messages:
- Significant surgical findings of endometriosis do not necessarily mean more pain
- There are likely different subsets of endometriosis with different implications for a patient’s pain
- Women with endometriosis may also have other impairments or factors that cause pain and these issues need to be treated, along with endometriosis, for better outcomes and less pain
- Some women have endometriosis and NO pain
Women with painful endometriosis process pain differently than women with non-painful endometriosis
Here is what is interesting: women with painful endometriosis showed different brain responses than women with non-painful endometriosis. Women with painful endometriosis experience repeated bouts of cyclical pain and are exposed to changing levels of pain. Studies show women with painful endometriosis are more sensitive to noxious stimuli and have amplified pain reactions to noxious stimuli than women who have non-painful endometriosis. 5,6
Another study showed that women with endometriosis had increased levels of neurotransmitters involved with pain and increased levels of these neurotransmitters facilitate communication with pain-modulatory networks in the brain. 7 The amount of connectivity between these areas increases with the amount of time pain is present. 7This is interesting because women typically go an average of seven to ten years without having a diagnosis, or therefore treatment for their pain. 1,8 As time goes on without a proper diagnosis or treatment, the areas of the brain that control pain are more active, and as women are exposed to repeated episodes of pain, they are becoming more sensitive to pain and are experiencing higher levels of pain than a woman who may not suffer from pain, even though both women may have the disease.
Endometriosis lesions are innervated and they cause inflammation, which sensitizes peripheral nerves. 9If it takes seven years to get diagnosed that is seven to ten years of painful periods. This will result in a sensitive nervous system. When women are diagnosed, excision or ablation surgery may be an option which may further sensitize irritated nerves.
What does this mean? Take home messages:
- Repeated episodes of pain can sensitize the nervous system.
- People with sensitized nervous systems will benefit from treating the nervous system in addition to eliminating the source of pain, surgery alone may not result in total pain reduction in most of these cases.
- The nervous system is very malleable, it changes in response to pain and it can also change back to a normal pain-free state when the triggers are removed
How do we know which patient is which? What do we do with this information?
Brain activity in women with painful endometriosis is different than women with non-painful endometriosis. 8This argues that we have to consider more than just the lesion as the generator of pain.
These women were then looked at pre/post surgery six months later and identified women with neuropathic pain (shooting, burning, electric pain) vs. nociceptive pain (sharp, aching, throbbing), and showed that women who had nociceptive pain had a decrease in their pain levels six months after surgery, while the group who had neuropathic pain actually had increased levels of pain six months post surgery. 8 What does this mean and how can it change clinical practice? It means that performing surgery or repeated surgeries (which is common) on women who have neuropathic pain, may be more harmful than beneficial.
One of the studies that was presented showed that in women who described their pain as neuropathic (versus nociceptive), had higher communication and connections between the areas of the brain that are active with pain. Considering that the nervous system can amplify pain levels, potentially it may be more important to separate the women by the type of pain versus the intensity of pain they describe. (8)
The PNS and CNS: how they work together and what else can influence pain.
A clinical picture
The pain may have started from a lesion in the periphery as soon as a woman gets her period. She may experience extremely bad periods but told “it’s just normal” or “it’s part of being a woman.” Considering the information presented, this woman may go many years with cyclical periods which we found out can cause central changes. Now, this woman had a peripheral source of pain, but the pain is now driven, or amplified, by the central nervous system.
Stress
One of the studies Dr. Vincent presented showed that cortisol levels were lower in women with painful endometriosis or painful periods compared to women who had non-painful endometriosis. 10 This was important because one area of the brain that is studied in all chronic pain conditions, the hypothalamic pituitary adrenal (HPA) axis, is altered in all chronic pain conditions. 10 This area has a lot of cortisol receptors and helps us to regulate our pain levels in times of stress. Cortisol is our “stress hormone” and kicks in that “fight or flight” response to help us get out of danger.
Dr. Vincent expanded on this a bit more, explaining that stress-induced analgesia is evolutionary, you cannot think about pain in your foot if you trying to run from danger. Researchers saw that not only the baseline level of cortisol but the change in cortisol levels after a stress response increases the amount of connectivity between the regions of the brain that help to inhibit pain. Cortisol influences inflammation and mood as well, and may explain the variation in women who have painful endometriosis vs. the women who have non-painful endometriosis. One study presented showed that women with painful endometriosis, as well as women that did not have endometriosis but had pelvic pain, had decreased cortisol levels. Additionally, women who had non-painful endometriosis had higher levels of cortisol, which can explain the variation in presentation.8
What does this mean?
Going back to the study mentioned above which demonstrated that women who had painful endometriosis or painful periods had lower cortisol levels compared to women who had non-painful endometriosis, this information tells us that certain groups of women respond to stress differently than others, and potentially the multiple symptoms associated with endo make it more complicated to discern what factors influence their pain.
We do know from this study that women who do not report pain have increased cortisol levels which activate the part of the brain that can help to inhibit pain. So, the question is – do they not have pain because they have better inhibitory mechanisms, or do they have better stress responses because they are not subjected to repeated cycles of pain and do not have as many changes in their CNS as someone with pain?
Comorbidities
Endometriosis is related to many other chronic conditions. In both inflammatory or endocrine disorders and chronic pain conditions, psychological distress is prevalent, and anxiety and depression are reported in 80+% in many studies.11 Studies have shown that if you just increase the anxiety levels in healthy women before giving them a painful stimulus, the intensity of the pain they experience will be higher. If you give them a stimulus that is sometimes painful or not, whether they perceive it as painful depends on the connectivity between various regions of the brain, and this connectivity is dependent on the level of anxiety at that moment.12So, anxiety can amplify pain, while depression also has other ways of amplifying pain.
What do we do with all this information?
Currently, simple analgesics, hormonal therapies, and surgery is the accepted model, and considering patient preference is key. Dr. Vincent suggests promptly treating any pain symptom, either endometriosis-related or comorbidity-related, and addressing any psychological distress will help to reduce the amount of burden on the CNS and result in better outcomes, especially if surgery is a consideration. The CNS may be the explanation between disease burden and symptoms, and may be the reason why women fail optimal surgery. It can also help explain why there are comorbid pain symptoms, and why they may have more hypersensitivity to stimuli. 8
As a pelvic floor physical and occupational therapists, I cannot prescribe medications, nor can I perform surgery or even make a medical diagnosis. However, we are at an advantage in treating this population of women because we see them more frequently than most other providers. We have a big role in educating patients about their symptoms and their disease and help them to understand and navigate all the medical jargon that even for us is hard to understand sometimes. We have a role in performing manual therapy and helping to reduce tissue restrictions, muscle tension, optimize breathing, creating home exercise programs with stretches and exercises, all of which can help to calm down the nervous system. To read more about the role of the physical and occupational therapy in treating endometriosis, please click here. From Dr. Vincent’s lecture, I feel that what I can do better in my clinical practice, and what we should all be doing as providers, is helping our patients to better understand the complexity of chronic pain and breaking down the information in ways that make more sense to our patients as well as discussing why we do what we do with them and how that can improve their outcomes.
We thank- Dr. Vincent for her great lecture! If you would like to view her presentation slides you may do so here, starting on page 85.
References:
- What is Endometriosis? – Dr Iris Kerin Orbuch | Los Angeles. (n.d.). Retrieved November 14, 2017, from https://www.lagyndr.com/endometriosis/what-is-endometriosis/
- Stratton, P., & Berkley, K. J. (2010). Chronic pelvic pain and endometriosis: translational evidence of the relationship and implications. Human Reproduction Update,17(3), 327-346.
- Vercellini, P., Fedele, L., Aimi, G., Pietropaolo, G., Consonni, D., & Crosignani, P. (2006). Association between endometriosis stage, lesion type, patient characteristics and severity of pelvic pain symptoms: a multivariate analysis of over 1000 patients. Human Reproduction,22(1), 266-271.
- Fauconnier, A., & Chapron, C. (2005). Endometriosis and pelvic pain: epidemiological evidence of the relationship and implications. Human Reproduction Update,11(6), 595-606.
- Bajaj, P. (2003). Endometriosis is associated with central sensitization: a psychophysical controlled study. The Journal of Pain,4(7), 372-380.
- He, W., Liu, X., Zhang, Y., & Guo, S. (2010). Generalized Hyperalgesia in Women With Endometriosis and Its Resolution Following a Successful Surgery. Reproductive Sciences,17(12), 1099-1111.
- As-Sanie, S., Kim, J., Schmidt-Wilcke, T., Sundgren, P. C., Clauw, D. J., Napadow, V., & Harris, R. E. (2016). Functional Connectivity Is Associated With Altered Brain Chemistry in Women With Endometriosis-Associated Chronic Pelvic Pain. The Journal of Pain,17(1), 1-13.
- Vincent, K. (2017, October 17). Endometriosis-associated pain. Why should we consider the central nervous system? Speech presented at IPPS 2017 and WCAPP in Renaissance hotel, Washington DC.
- Chiu, I. M., Hehn, C. A., & Woolf, C. J. (2012). Neurogenic inflammation and the peripheral nervous system in host defense and immunopathology. Nature Neuroscience,15(8), 1063-1067.
- Vincent, K., Warnaby, C., Stagg, C. J., Moore, J., Kennedy, S., & Tracey, I. (2011). Dysmenorrhoea is associated with central changes in otherwise healthy women. Pain,152(9), 1966-1975.
- Sinai, N., Plumb, K., Cotton, L., Lambert, A., Kennedy, S., Zondervan, K., & Stratton, P. (2008). Differences in characteristics among 1,000 women with endometriosis based on extent of disease. Fertility and Sterility,89(3), 538-545.
- Ploghaus A., Narain C., Beckmann CF. et al. (2001). Exacerbation of pain by anxiety is associated with activity in a hippocampal network. J Neurosci.15;21(24):9896-903.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
Great article
The information about calming down the central nervous system is so important when dealing with chronic pain and this is hardly ever dealt with by mainstream medicine. Unfortunately women still think that if you mention anxiety, stress and depression in relation to pain you are suggesting that it’s “all in their head”. I’m a registered nurse in the UK working in general practice and I also have been dealing with chronic pelvic pain myself for many years (endometriosis, vulvodynia, irritable bowel syndrome, interstitial cystitis). I have seen a massive improvement in my symptoms over the past year after undertaking physiotherapy and dealing with the mind/body connection in relation to the pain. This has included attending a mindfulness for health course, undertaking a ‘healing female pain’ online course and reading Moseley and Butlers work on pain/chronic pain and putting their advice into practice.
Thank you for such a great article and all the work you do. This site and reading the book ‘pelvic pain explained’ was so helpful to me during my quest to heal.