
By Cambria Oetken, PT, DPT
Background
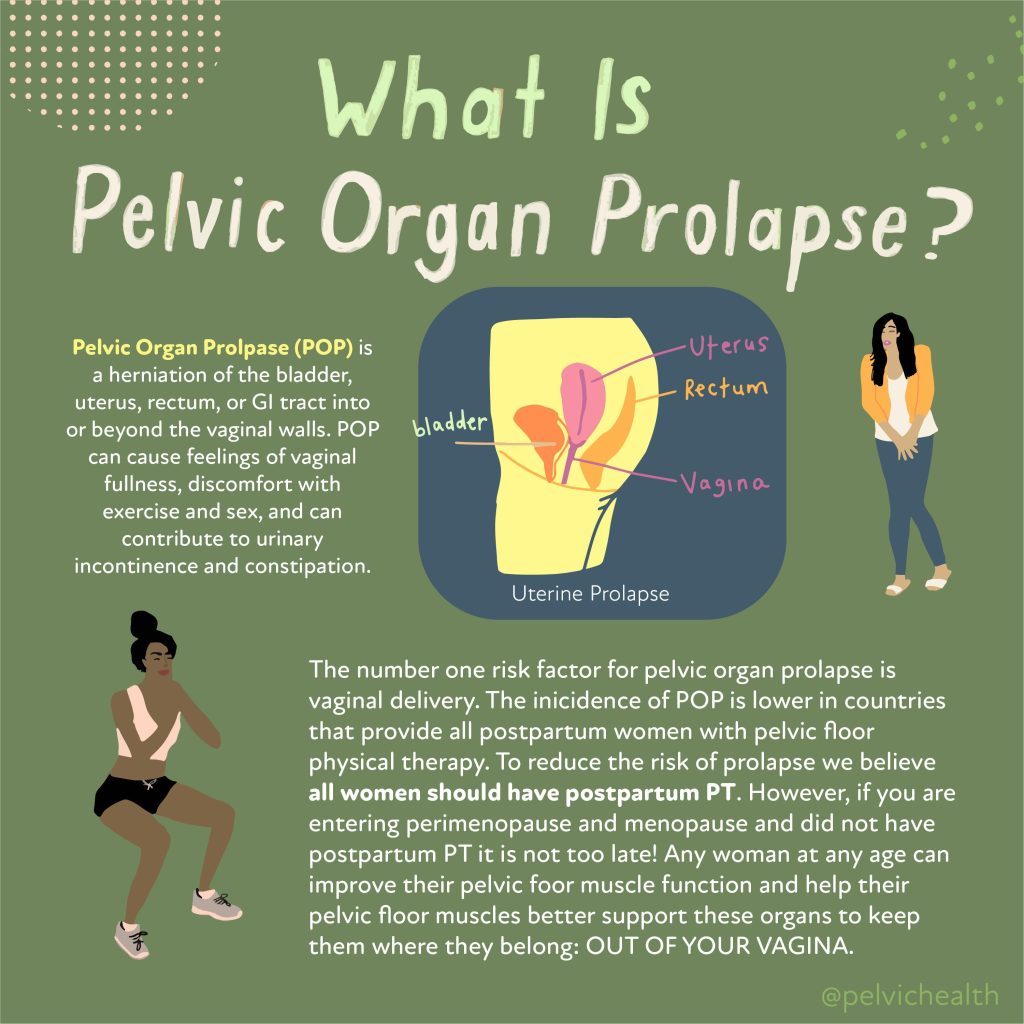
Diane is a 66-year-old woman with a history of three vaginal deliveries. She came to PHRC with a significant history of pelvic floor pain, muscle spasms, urinary incontinence, pain with intercourse, and muscle weakness. Diane had undergone multiple pelvic reconstruction surgeries for pelvic organ prolapse (POP), the most recent being a total hysterectomy and prolapse reconstruction. In addition to her pelvic surgeries, Diane also underwent a partial mastectomy for breast cancer and radiation treatment.
After several years of significant health challenges, Diane felt weak, unable to lift her new grandson, care for her granddaughter, or participate in her very active role as a lead nurse.
Primary Concerns:
- Urge urinary incontinence
- Pelvic floor pain
- Muscle weakness and fatigue
- Pressure and heaviness in the pelvic region
- Pain with penetrative intercourse
Diane’s Goals:
- Gain control over bladder to reduce incontinence episodes
- Return to pain-free penetrative intercourse with her partner
- Improve muscle strength to lift her grandson and ride her beach cruiser while camping
- Paddleboard with her husband
- Decrease pelvic floor pain, pressure, and heaviness
- Be able to push, pull, and lift patients as a nurse (with assistance from a coworker)
Physical Findings:
Upon examination, physical findings revealed
Myofascial impairments:
- Medial thigh and hip flexors (iliacus)
- Deep hip rotators (obturator internus and piriformis)
- Anterior and medial thigh
- Gluteal muscles
Additional findings:
- Difficulty performing a “pelvic drop” with limited range of motion
- Decreased pelvic floor strength (score of ⅖)
- Poor intra-abdominal pressure management with reduced transverse abdominal activation
Plan and Outcome:
The physical findings above likely developed following a period of deconditioning and a sedentary lifestyle due to pelvic reconstruction surgeries, recovery from radiation, and the mastectomy.
To start, we provided education and habit changes for Diane to improve her urinary control and function. These included:
- Toilet mechanics: Leaning forward after voiding to improve bladder emptying
- Urgency suppression strategies: Using the “fake out” technique to prevent incontinence episodes when unlocking the front door
- The “Fake Out” Technique: This is helpful for what is known as “Latchkey” incontinence, this occurs when you get the sudden urge to pee or have urinary incontinence when arriving home or putting your key into the door to enter your home. A few ways we can combat this to psych our brain and bladder:
- Fake out strategy 1: When approaching your door, turn around and walk away. Take a 5 deep diaphragmatic breaths and slowly walk back up to your door to enter your home.
- Fake out strategy 2: Approach your door and stop. Perform 3 deep squats inhaling down into the squat to relax your pelvic floor and exhale as you stand up out of the squat. This can help relax the pelvic floor muscles before entering.
- Fake out strategy 3: As you approach your door perform 3-5 pelvic floor contractions or “kegels”. This will contract your pelvic floor and inform your bladder to relax and let it know we are not urinating right now! Then slowly enter your home.
- Try these 3 strategies and see how far inside your home you can make it. IF you have completely suppressed the urge, great! If you continue to have an urge inside feel free to walk to the restroom to void if needed.
- The “Fake Out” Technique: This is helpful for what is known as “Latchkey” incontinence, this occurs when you get the sudden urge to pee or have urinary incontinence when arriving home or putting your key into the door to enter your home. A few ways we can combat this to psych our brain and bladder:
- Prolapse relief positions: Elevating the hips and legs to reduce pressure and discomfort
- Postural awareness: Adopting a stacked posture at work, avoiding glute clenching, and preventing upper abdominal gripping
- Vaginal tissue health: Using vulvar moisturizers to address dryness
- Proper transfer training at work: Focusing on exhaling during exertion, whether lifting, pushing, or pulling patients

After just a few sessions, Diane showed dramatic improvement:
- No longer experienced leaks at work
- No incontinence when walking into her front door
- Reduced pressure and heaviness in the pelvic region by the end of the day
To continue progressing, Diane’s treatment included a functional strength program with the following:
- Bridges with adductor squeeze for pelvic floor engagement
- Mobility and stretching routine, including adductor rock-backs, deep hip rotator stretching, and medial thigh foam rolling
- Pelvic floor proprioception techniques, such as sidelying proprioception of the pelvic floor and using a rolled towel for pelvic floor muscle awareness
- Strength exercises: Deadlifts, RDLs, Pallof presses (with and without rotation), and D1 extension on a blue foam mat to simulate paddleboarding
- Slider lunges in multiple directions to improve functional strength
Additional treatments included:
- Manual therapy: Myofascial manipulation and connective tissue mobilization to restore normalcy to medial thighs and deep rotators
- Motor control training: Focused on improving pelvic floor drops and strengthening the pelvic floor muscles
Through her commitment and consistent practice of her home exercise program, Diane reported:
- No longer needing pads or experiencing incontinence episodes
- Increased confidence in herself
- Successfully paddleboarding three days in a row on a camping trip
- Being able to ride her bike during the trip
- Feeling stronger and more capable
- Comfortably lifting and caring for her 35lb grandson
- No pelvic floor spasms or pain
- Returning to pain-free intercourse with her partner
Objective Findings: Diane showed significant improvements in pelvic floor strength, with her strength score increasing from ⅖ to 4/5, demonstrating a substantial recovery in strength
Final Thoughts: Diane’s dedication to her rehabilitation program, combined with targeted treatments and exercises, allowed her to overcome significant challenges and return to the activities she loves. Her story is a great example of how pelvic floor therapy can restore both function and quality of life.
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
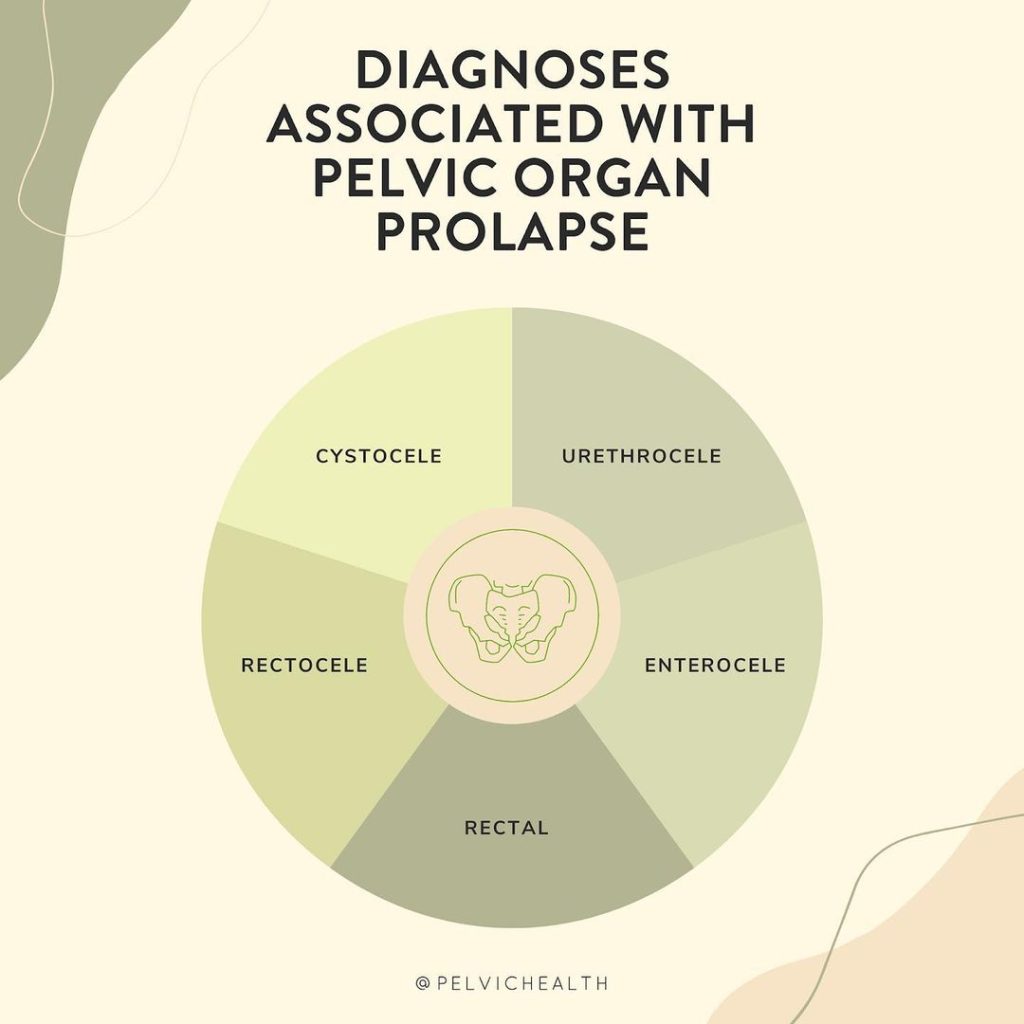
tags: prolapse, pelvic organ prolapse, pelvic organ, anterior vaginal wall prolapse, pelvic floor exercises, pelvic muscles, posterior vaginal wall prolapse, uterine prolapse