By Cambria Oetken, DPT, PHRC Westlake Village
Our sexual medicine experts have written a review shared in the International Society of Sexual Medicine Journal in regards to Clitoral Adhesions through a literature review written by Jennifer P. Romanello, Monica C. Myers, Elsa Nico, and Rachel S. Rubin. If you have not already, check out our recent blog on “How High is Your Clitoris IQ?” for additional information on clitoral health. Below we will be discussing all things clitoral diagnoses, particularly adhesions and treatment options.
What are clitoral adhesions?
Clitoral adhesions refer to the pathological attachment of the clitoral hood to the clitoris, often resulting in discomfort or functional impairments. More specifically, the clitoral prepuce (the hood) adheres to the glans clitoris making it difficult to fully retract the hood in order to expose the entirety of the clitoris. The condition is actually more common than we had previously believed and can have significant clinical and psychosocial implications, particularly regarding sexual function and quality of life.
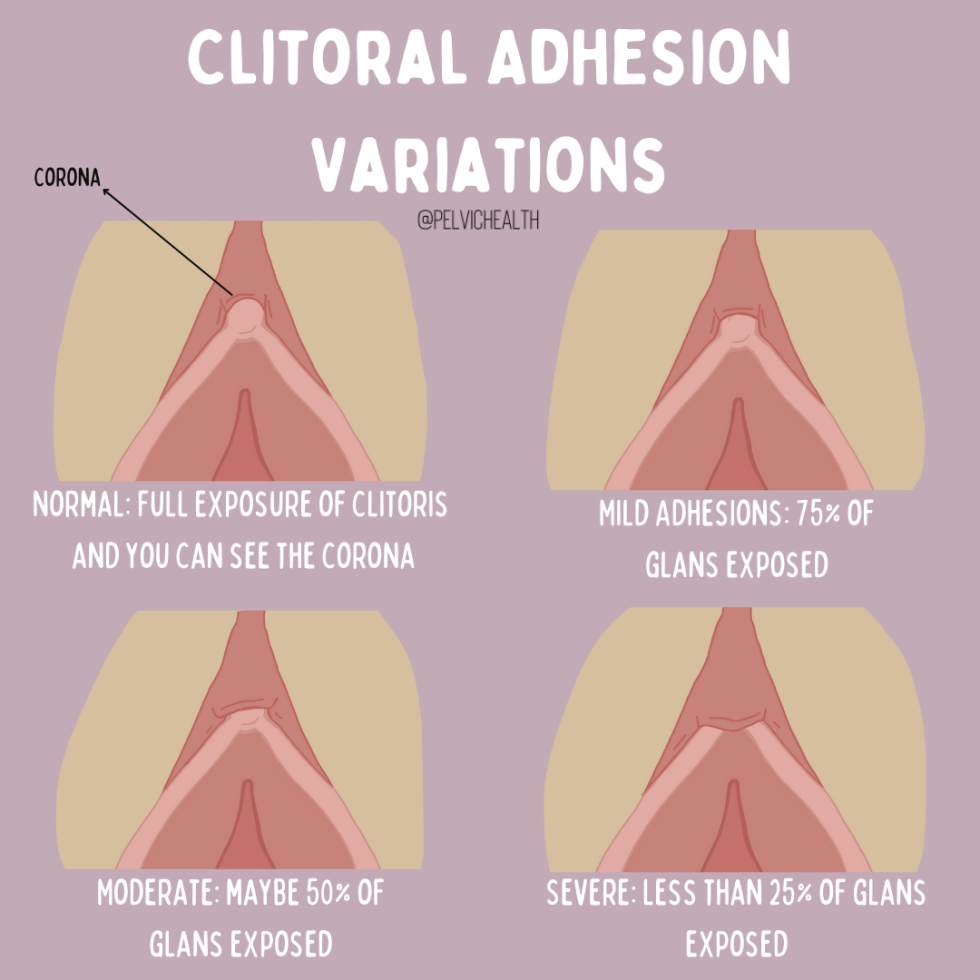
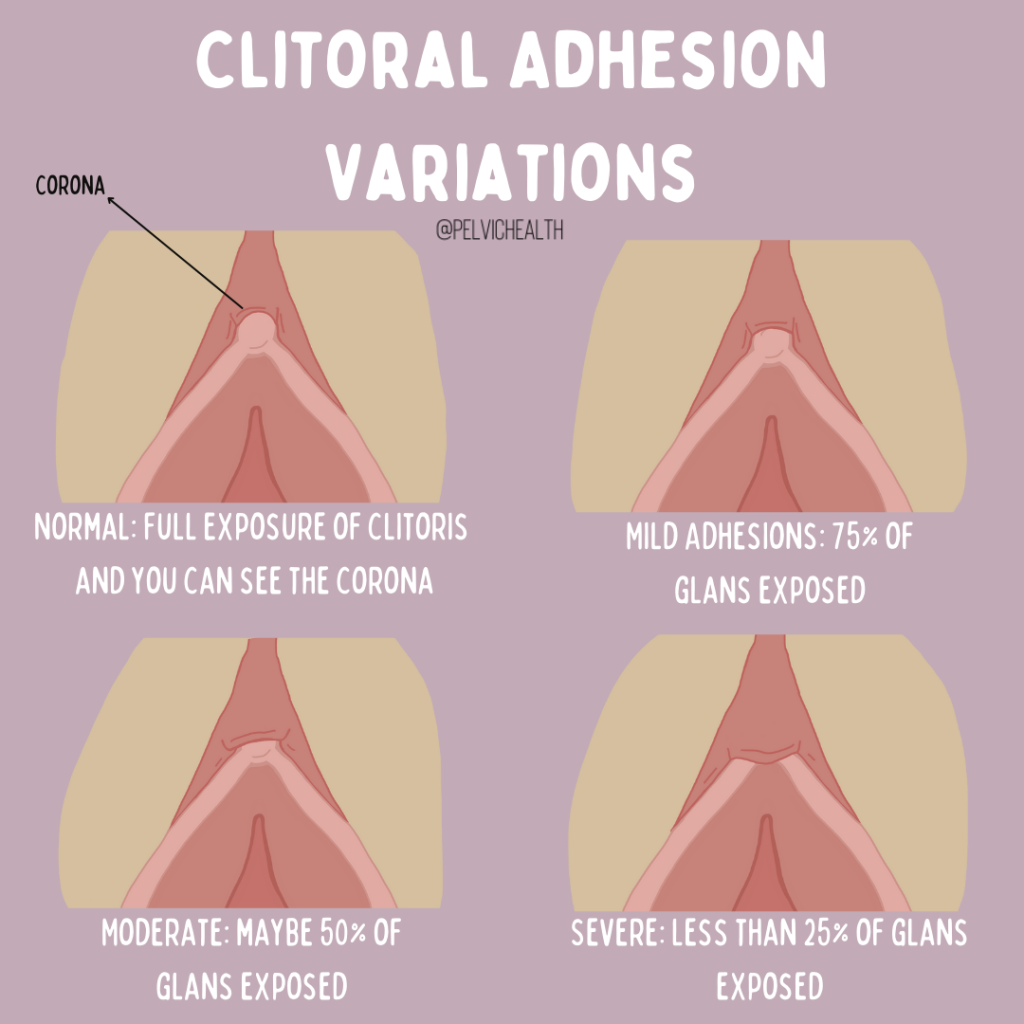
Degrees of Clitoral Adhesions
There are different variations in adhesions based on how much of the glans is hidden by the prepuce. Adhesions can be categorized as mild meaning there is more than 75% exposure of the glans, moderate is 25% to 75% exposure of the glans upon retraction and severe adhesions indicating less than 25% of the glans is exposed. The value in understanding and being aware of adhesions is due to symptoms that can be associated with it including pain, sexual dysfunction, difficulty with arousal and orgasm. These symptoms can be very impactful on someone’s quality of life and should therefore be acknowledged, understood and evaluated by providers.
What contributes to clitoral adhesion in the first place?
Adhesions can start as a result of scarring, whether from vulvar lichen sclerosus or lichen planus as well as trauma or physical injury to the area. Examples of injury or trauma include female genital mutilation or cutting FGM/C that can take place in specific cultural traditions. Other causes include inflammation, recurrent infections (STIs or bacterial vaginosis), yeast infections that are vaginal and/or cutaneous; however, we know so much more research is needed.
The vulva and clitoris are hormonally sensitive structures, meaning they are dependent on androgen and estrogens for normal function. Medications and phases of life can lead to hormonal deficiencies which can result in the clitoris reducing in size. One theory regarding adhesions and pearls is that altered anatomic size may contribute to smegma or inflammatory agents accumulating under the hood and causing scarring. Situations that can lead to hormonal deficiencies include medications such as oral birth control pills, hormonal suppressant medication for endometriosis, women who are breast feeding, and women who are in perimenopause and menopause.

Interestingly, when reviewing patients who presented with pain at the clitoris (clitorodynia), clitoral adhesions and keratin pearls seemed to be a concomitant of Genitopelvic pain disorders such as overactive pelvic floor muscle dysfunction, pudendal neuralgia, interstitial cystitis/painful bladder syndrome and provoked Vestibulodynia related to a hormonal factor.
Clinical Presentation
Patients with clitoral adhesions may or may not have physical symptoms however primary symptoms can include pain during sexual activity (dyspareunia), decreased sexual arousal or orgasm, general discomfort or irritation in the genital area, and clitoral hypersensitivity (increased sensation that can be uncomfortable) or hyposensitivity (reduced sensation). Additional presentations can include keratin pearls or smegma build up. Due to the closed compartment of the adhesions it makes draining more difficult to clear smegma which is composed of sebum and specific epithelial cells. Keratin pearls on the other hand are firm, small masses of dense keratinization within layers of squamous cells in the dermis that can contribute to pain especially if it becomes inflamed or infected. It is thought that a keratin pearl can feel like a sensation similar to “a grain of sand in the eye”.
If you are experiencing any of these symptoms, it is best you share these concerns with your provider and/or your sexual medicine expert. You can also check our recent article“How High is Your Clitoris IQ?” on how to perform a clitoral examination on yourself.
Treatment
Non-Surgical Options:
Nonsurgical Lysis Procedure: Performed in office using a local anesthetic that consists of stretching the prepuce (hood) to expose the clitoris and remove any smegma or keratin pearls. Research shares that a majority of patients who have this procedure report improved pain, arousal, or ability to achieve orgasm
Topical Corticosteroids: Typically used in the treatment of patient with lichen sclerosus such as clobetasol are commonly used. This works to decrease inflammation however can not correct scarring that is already present. Suggestion of corticosteroid use with the lysis procedure to address scarring has been considered as a more comprehensive strategy.
Local Hormones: While using topical hormone cream requires further research, a risk factor for clitoral adhesions is insufficiencies of sex hormones. Topical estradiol and/or testosterone have been utilized in managing adhesions.
Hygiene Measures and Retraction: Self retraction of the clitoral hood is typically recommended following a lysis procedure in order to prevent recurrence and is also a wellness measure that can be practiced daily to maintain clitoral hood mobility. Ensuring you do not use harsh soaps or chemicals to clean the area is recommended, warm water is enough to suffice. Some suggestions on petroleum jelly have been recommended in the past but have limited research.
View this post on Instagram
Carbon Dioxide Lasers: This is considered a novel procedure based on previous research and results that has been somewhat successful with patients in addition to topical hormone usage. This laser helps to perform a surgical correction of the adhesions using fine dissection of scar tissue.
Surgical Option:
Surgical Lysis Procedure: A surgical technique that is more invasive than an in office lysis procedure but has shown great success and patient satisfaction. Notable increases in clitoral sensation and decreased pain with intercourse were highly reported following the procedure.
Pelvic Floor Physical/Occupational Therapy is a Treatment Option!
People suffering from sexual dysfunction and sexual pain should undergo a pelvic floor evaluation with a skilled provider to rule in or out connective tissue, muscle, and peripheral nerve contributions. Physical/Occupational therapy and medical management go hand in hand to help people restore comfort and pleasurable sexual experiences!
Conclusion
It is important to note the relevance of this condition as it is showing up in approximately 22% of women who are seeking consultation for sexual dysfunction and in 33% of female college students during routine examinations. The article highlights the importance of clitoral adhesion consideration in the clinical evaluation of pain and sexual dysfunction in multiple settings. Clitoral exams should be a routine part of pelvic exams in order to expedite proper diagnosis and treatment.
Reference
Romanello JP, Myers MC, Nico E, Rubin RS. Clitoral adhesions: a review of the literature. Sex Med Rev. 2023 Jun 27;11(3):196-201. doi: 10.1093/sxmrev/qead004. PMID: 36973166.
Blog Resources
Interstitial Cystitis/Painful Bladder Syndrome
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok
tags: persistent genital arousal disorder, clitoral phimosis, severe clitoral adhesions, sexual health, clitoral adhesions occur, glans clitoris, clitoral prepuce, women’s health providers, sexual arousal, sexual pleasure