
By Jandra Mueller, DPT, MS, PHRC Encinitas
As menstruating people, you would think that we would understand what a period is, the purpose of it, and all of the information it can give us. Unfortunately, we do not, and this is not okay. Our periods are more than a sign we are not pregnant, more than an inconvenience, more than something we have to just deal with. Understanding what they are and why we have them can provide us with significant information about our health. As Lara Briden, ND says, “it’s our monthly report card about our health.”
In today’s blog, I discuss everything you should have learned in sixth grade, but didn’t, about what is normal. Part two and three of this blog series will talk about all the issues when you do not have a regular or healthy menstrual cycle, the various things that can affect your cycle like hormonal birth control, treatment considerations, and what alternative options are available.
Starting from the beginning: menarche.
In December of 2015, ACOG released a committee option paper titled “Menstruation in girls and adolescents: Using the menstrual cycle as a vital sign.” This. Is. Huge. It is so important, first to know what is normal, and what is normal varies depending on which cycle of life we are in. For example, when you first start menstruating, cycle length can be longer than in your adult years because your hypothalamic-pituitary-ovarian axis (HPA axis) is just establishing itself and hormones fluctuate. You may have a cycle that is anywhere between 21 and 45; whereas longer than 35 days in an adult is typically abnormal. If you ask an adult figure in your life, who may not understand the menstrual cycle because they weren’t educated either, they may think something is wrong, take you to the doctor (probably your primary care physician) and you may be placed on hormonal birth control to ‘regulate’ your cycle. NO! This. Is. Normal!
Typically, normal menarche (the start of menstruation) begins on average at the age of 12-13 years old in well-nourished populations and in developed countries. Changes to this norm could be due to environmental factors, socioeconomic conditions, nutrition, and access to preventive health care. Menarche typically begins two to three years after ‘thelarche’ which is the development of breast buds which can be as early as age eight; and in most this occurs menarche begins by the age of 15 (ACOG, 2015).
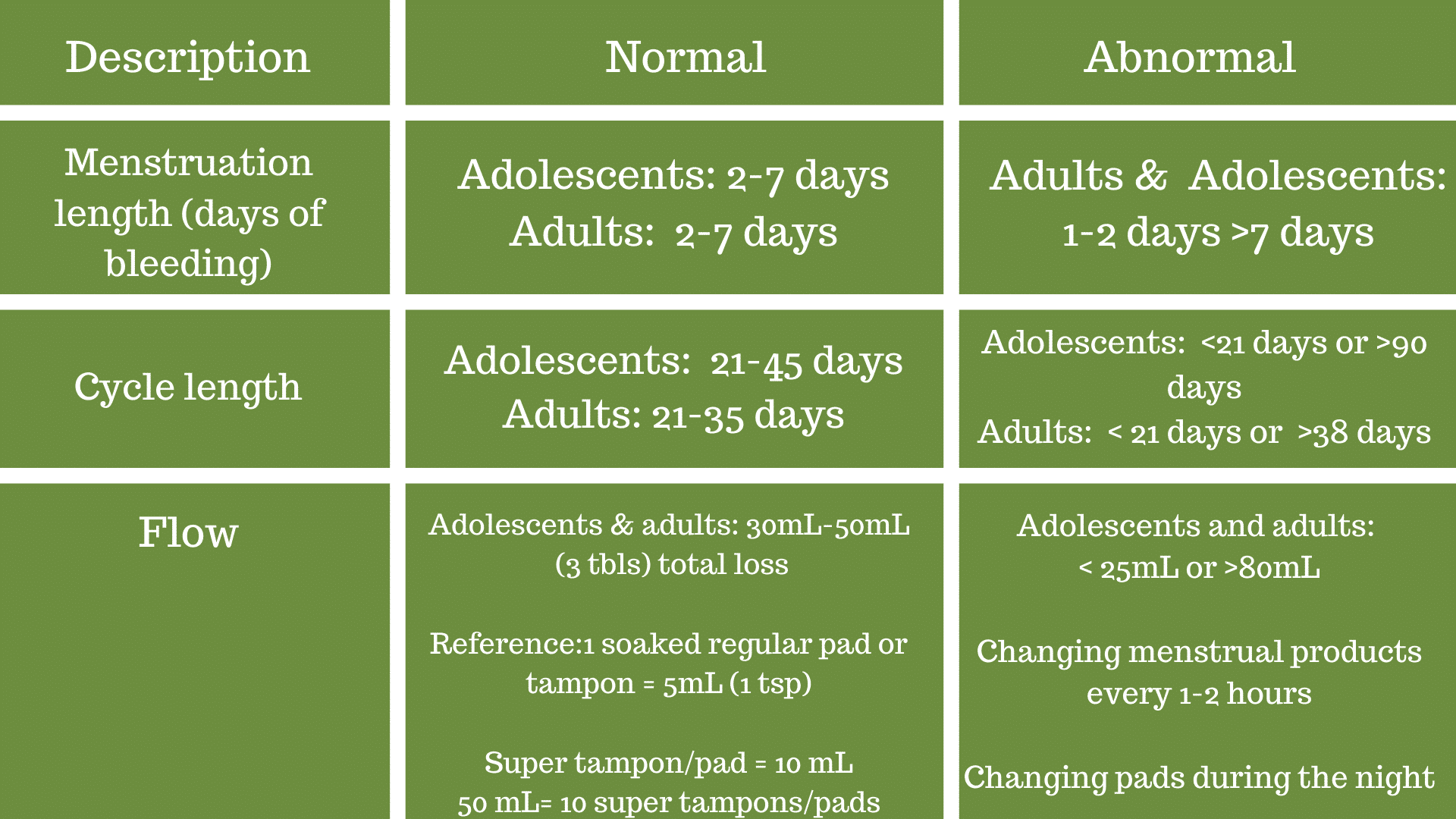
Your menstrual cycle takes about three years to really establish itself. Cycles typically are 21 to 35, although they can fall out of that range and still be normal, and most menstruate (bleed) for about two to seven days (ACOG, 2015). As adults, normal menstrual cycles are between 21-35 days. The amount of flow can vary, but typical blood loss is 30 mL. Blood loss more than 80 mL is considered chronic blood loss and is associated with anemia.
How to measure your blood loss in real life. Dr. Lara Briden gives a great example in her book “The period repair manual” where she presents how to count your menstrual products.
Counting menstrual products:
1 soaked regular tampon or pad = 5 mL (1 tsp)
1 soaked super tampon/pad = 10 mL (2 tsp)
50 mL blood loss = 10 soaked regular product or 5 soaked super products
*These are the total products used, not each day
Recap: what is abnormal?
- Adolescent girls should be evaluated if they go longer than three months (90 days) between periods.
- Bleeding for more than seven days
- Changing menstrual products every one to two hours
- Changing pads during the night
What is a period?
Often, the terms periods and cycles are used in the wrong context. Periods are the time we are bleeding (menses) and our menstrual cycle is the entire time we are bleeding and not bleeding, until the cycle repeats itself. Periods are called periods because it comes periodically at approximately monthly intervals. The first day of actual bleeding (not spotting) is day one of your menstrual cycle. Most people bleed on average three to five days.
The phases of your cycle
A cycle is classified as day one of heavy bleeding to day one of your next period. Heavy bleeding is not the light spotting or ‘brownish’ discharge that may occur right before your period actually starts, this spotting is actually left-overs from the previous cycle. 28days is the average cycle for adults, but can be anywhere from 21 to 35 days and still be normal.
The Follicular Phase: The first phase of your cycle is called the follicular phase which is approximately two weeks. In this phase, your ovarian follicles are entering the final stages of development, and there is one dominant follicle that will release an egg at ovulation. Typically this phase can last anywhere from seven to 21 days (Briden, 2018).
In this phase a few of your follicles enter their final stages, although they began this process long before. Dr. Briden points out, it takes about one hundred days (~three months) for an ovarian follicle to reach maturation. During this phase, a hormone from your pituitary gland is releasing follicle-stimulating hormone (FSH) and luteinizing hormone (LH) which help them to reach ovulation and produces the sex hormone estradiol (Briden, 2018). Estradiol is the primary estrogen in premenopausal women, and plays a significant role in your health and is involved with mood, bone health, and insulin resistance. It helps to promote the growth of the uterine lining in anticipation of pregnancy. During this time where estradiol dominates, you may see a change in your cervical mucus in your vaginal discharge. This type of mucus tends to be creamy, wet, and slippery (Briden, 2018). Your vaginal discharge is a combination of this mucus, shed cells from your vaginal wall, and healthy bacteria (Briden, 2018).
Ovulation is the next phase and lasts one day. The dominant follicle releases an egg that is ready to be fertilized or be released along with the endometrium during your next period.
The luteal phase is the last phase and lasts between 10-16 days. This stage is very important and it only happens if you ovulate. Only then, will you also produce progesterone. What happens in this phase is that the follicle that released the egg begins to change into a gland that starts to secrete progesterone. Progesterone is sometimes referred to as “the pregnancy hormone” that dominates during pregnancy. If you are not pregnant this hormone still plays a vital role in your health such as balancing estrogen, breast cancer prevention, and increasing your body temperature (which is the basis of measuring your basal temperature in the fertility awareness method). Other benefits of progesterone are reducing inflammation, promoting sleep, and calming the nervous system (Briden, 2018).
Why ovulation is important
Ovulation is important because it is the event that the follicle has prepared 100 days for. This means that something that was ongoing with your health three months prior may show up now (Briden, 2018). This could be inflammation, poor nutrition, stress, etc. The corpus luteum, which turns into the gland that secretes progesterone has to live a healthy life so that it can not only release the egg, but then shift into essentially a completely different structure with its own blood supply in just a short amount of time (Briden, 2018). If it is unhealthy, it may not release an egg at all or it may only produce a small amount of progesterone, which could cause some problems as we will discuss in a later blog post.
The fate of the egg: Period or Pregnancy
In healthy menstrual cycles, your fertile time is the three (sometimes five) days before you ovulate and the day of ovulation. The reason for this is because the cervical mucus you should see around the time of ovulation, also known as the fertile mucus, was stimulated by the estradiol from the follicle that just released that egg. It is the perfect environment for sperm, and sperm can survive for a few days, but the egg can only survive for twenty-four hours. Remember, this is in reference to normal, healthy menstrual cycles only. Your fertility window can change if your cycle is abnormal and you do not follow a normal menstrual pattern. It may also change if there has been significant stressors (perceived stress is important, diet, exercise, illness etc. can also affect this normal pattern). After the egg is released, its fate is either pregnancy or to be released out of your body during your period. This cycle repeats itself every month until you begin to approach menopause, get pregnant, or have an underlying health condition.
Click here to continue reading part 2 of this blog!
References:
- ACOG Committee Opinion No. 651: Menstruation in Girls and Adolescents: Using the Menstrual Cycle as a Vital Sign. Obstet Gynecol. 2015;126(6):e143-e146.
- Briden L, Prior JC. Period Repair Manual: Natural Treatment for Better Hormones and Better Periods. Place of publication not identified: Greenpeak Publishing; 2018.
______________________________________________________________________________________________________________________________________
Are you unable to come see us in person? We offer virtual physical and occupational therapy appointments too!
Due to COVID-19, we understand people may prefer to utilize our services from their homes. We also understand that many people do not have access to pelvic floor physical and occupational therapy and we are here to help! The Pelvic Health and Rehabilitation Center is a multi-city company of highly trained and specialized pelvic floor physical and occupational therapistss committed to helping people optimize their pelvic health and eliminate pelvic pain and dysfunction. We are here for you and ready to help, whether it is in-person or online.
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. The cost for this service is $85.00 per 30 minutes. For more information and to schedule, please visit our digital healthcare page.
In addition to virtual consultation with our physical and occupational therapistss, we also offer integrative health services with Jandra Mueller, DPT, MS. Jandra is a pelvic floor physical and occupational therapists who also has her Master’s degree in Integrative Health and Nutrition. She offers services such as hormone testing via the DUTCH test, comprehensive stool testing for gastrointestinal health concerns, and integrative health coaching and meal planning. For more information about her services and to schedule, please visit our Integrative Health website page.
PHRC is also offering individualized movement sessions, hosted by Karah Charette, DPT. Karah is a pelvic floor physical and occupational therapists at the Berkeley and San Francisco locations. She is certified in classical mat and reformer Pilates, as well as a registered 200 hour Ashtanga Vinyasa yoga teacher. There are 30 min and 60 min sessions options where you can: (1) Consult on what type of Pilates or yoga class would be appropriate to participate in (2) Review ways to modify poses to fit your individual needs and (3) Create a synthesis of your home exercise program into a movement flow. To schedule a 1-on-1 appointment call us at (510) 922-9836
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Like us on Facebook,
Subscribe to our YouTube Channel,
and follow us on Twitter, Instagram and Pinterest!
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.