
Putting down the prescription pad: The opioid epidemic and pelvic pain
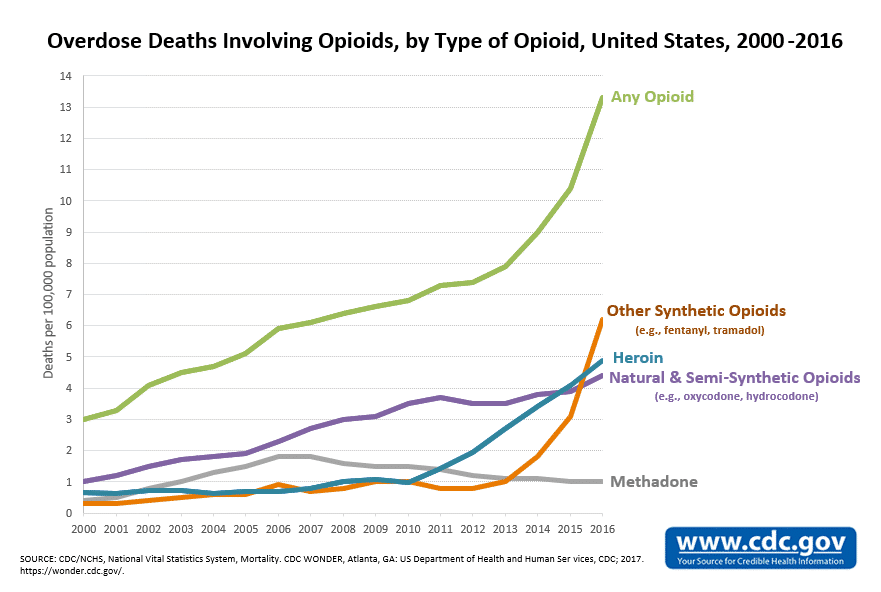
It should be a surprise to no one that we are in the middle of a serious, nationwide opioid epidemic. And to top that off, a crisis on opioid overdose. Did you know that on average 115 Americans die each day from opioid overdose?2 In October 2017, President Trump declared the opioid crisis a public health emergency and has since been developing strategies to combat this crisis.1 It was just a week ago that the New York Times published a story on an opioid epidemic that has been ongoing for over 150 years in the United States. Unfortunately, the rise of opioid use and overdose has been drawn back to the prescription pad; especially when you consider that there has been no change in the amount of pain reported by Americans since 1999 while the amount of opioids being prescribed has quadrupled.3
As a pelvic health physical and occupational therapists, I am all too familiar with the great lengths to which people will go for relief from chronic pain. As I continue to evaluate and treat patients who have been suffering with undiagnosed pain for over 10 years and I see opioids in their medical history, it brings me to ask the following questions:
Are opioids an appropriate treatment for pelvic pain?
What can I do to help fight the opioid epidemic?
To answer my first question…
There is no research to definitively support or negate opioids as a treatment for pelvic pain. This is an ongoing debate in the medical community, particularly when it comes to opioids and chronic, neuropathic pain. Opioids have been shown to effectively provide short-term relief for acute pain; however, the evidence is limited in its benefits for chronic pain. This leaves us to consider the individual, risks, benefits, and our clinical expertise.
In the Urological and Gynaecological Chronic Pelvic Pain textbook, Dr. Robert M. Moldwin, MD reports that opioids can effectively treat chronic pelvic pain in the short-term by altering pain perception through afferent pathways of the central nervous system.4 NMDA-antagonizing opioids have been shown to lower nerve hyperexcitability, which is useful considering that persistent, neuropathic pain involving the pudendal nerves can lead to hyperexcitability in the nociceptors. However, opioids do not affect neuronal firing or transduction, which partially explains the temporary nature of opioid efficacy and will not address the neuroproliferative component of chronic, neuropathic pain.
In short, they can help reduce the pain intensity and give short-term relief but not effectively treat pain long-term. Opioids are best utilized with other therapies. The authors make a point to discourage monotherapy treatment with opioids and rather use adjunct therapist in combination with opioid prescriptions.
Opioids for chronic pelvic pain come with some pretty heavy risks like tolerance, dependence, and depression;5 side effects we see time and time again in the clinic. However, some of the other side effects gravely affect patients with pelvic pain. For one, these medications cause constipation, which is typically a known cause and effect of pelvic floor dysfunction, and pelvic pain (read more about this here). This can lead to more dysfunction and more pain. Opioids also cause decreased androgen production,4 leading to reduced levels of estrogen and testosterone which are risk factors for vestibulodynia, erectile dysfunction, and depression. Testosterone also helps our body tolerate and manage pain,5 which can lead to the downward spiral of more intense pelvic pain. Lastly, increased sensitivity to pain is listed as a side effect. Why would we recommend a medication that causes more pain and sensitivity in an area that is already so painful and sensitive?
If you weigh the risks and benefits, opioids are not an appropriate medication for pelvic pain when you consider that most pelvic pain is chronic (lasting >12 weeks). The CDC advises nonopioid therapy for chronic pain outside of active cancer, palliative, and end-of-life care.7 We have a whole laundry list of treatments that have evidence to support their efficacy of treating chronic pelvic pain that does not include opioids. These include:6
- Neuromodulators/neuromodulation
- Nerve blocks
- Physical therapy
- Dry needling
- Trigger point injections
- Cognitive behavioral therapy
- Behavioral modifications
- Diet modifications
So, what can I do to help this epidemic?
The best thing I can do is stay information on this topic and share my ever-growing knowledge with my patients in the clinic.
Since we know this epidemic is being perpetuated by prescriptions, I turn to the CDC’s Guidelines for Prescribing Opioids for Chronic Pain7. Here are a few highlights from the guidelines:
- Opioids are not first-line or routine therapy for chronic pain
- Establish and measure goals: the goal is to improve function not just pain
- The clinician should discuss risks, benefits, and role of the patient and provider
- Prescribe the lowest effective dose of immediate-release opioids
- Long-term use is discouraged; opioids are rarely needed longer than seven days for acute pain
- Clinicians should avoid prescribing pain medication and benzodiazepines concurrently
They also have a nifty handout version and mobile app.
The U.S. Department of Health and Human Services has a 5-point strategy to combat the opioid crisis.8

As physical and occupational therapistss, we can assist in better prevention of addiction and better pain management. We spend ample time to get to know our patients, understand their lifestyle, their limitations, and their goals. Inquiring about medications on the evaluation is key to recognizing opioid use. Communicating with their primary care physicians and healthcare team can reduce risk for abuse and overdose. Educating the community about more effective and appropriate treatments for chronic pain can reduce the risks associated with this epidemic. Even if we do not hold the prescription pad, we can still be a key player in the fight against opioids.
Patient and Provider Resources:
- CDC.gov
- HHS.gov
- Drugabuse.gov
- CrisisNextDoor.gov
References:
- The United States Government. The White House (2018, May 24). The opioid crisis. The United States Government. Retrieved from http://www.whitehouse.gov/opioids/.
- Center for Disease Control and Prevention (2017, Aug 30). Opioid overdose. Retrieved from http://www.cdc.gov/drugoverdose/epidemic/index.html.
- Center for Disease Control and Prevention (2017, Aug 30). Understanding the epidemic. Retrieved from https://www.cdc.gov/drugoverdose/epidemic/index.html
- Moldwin, R. (2017). Urological and gynaecological chronic pelvic pain : current therapies. Cham, Switzerland: Springer.
- White, D.H., Robinson, T.D. (2015). A novel use for testosterone to treat central sensitization of chronic pain in fibromyalgia patients. International Immunopharmacology, 27, 244-248.
- Prendergast, S. & Rummer, E. (2016). Pelvic pain explained : what everyone needs to know. Lanham: Rowman & Littlefield.
- Center for Disease Control and Prevention (2017, Aug 29). Factsheet CDC guideline for opioid prescription for chronic pain. Retrieved from
- U.S. Department of Health and Human Services (2018, May 24). Help, resources and information: national opioids crisis. Retrieved from https://www.hhs.gov/opioids/.
- Center for Disease Control and Prevention (2017, Aug 29). Prescription opioids. Retrieved from https://www.cdc.gov/drugoverdose/opioids/prescribed.html.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Can you tell me who treats physical Therapy pelvic pain in San Diego, I would like to know. Thank you
Hi Elizabeth,
We recommend Cindy Furey at Comprehensive Therapy Services, 858-457-8419.
Regards,
Admin