Let’s talk SIBO
SIBO stands for Small Intestine Bacterial Overgrowth; bacteria that is an overgrowth of the normal bacteria in your small intestine.

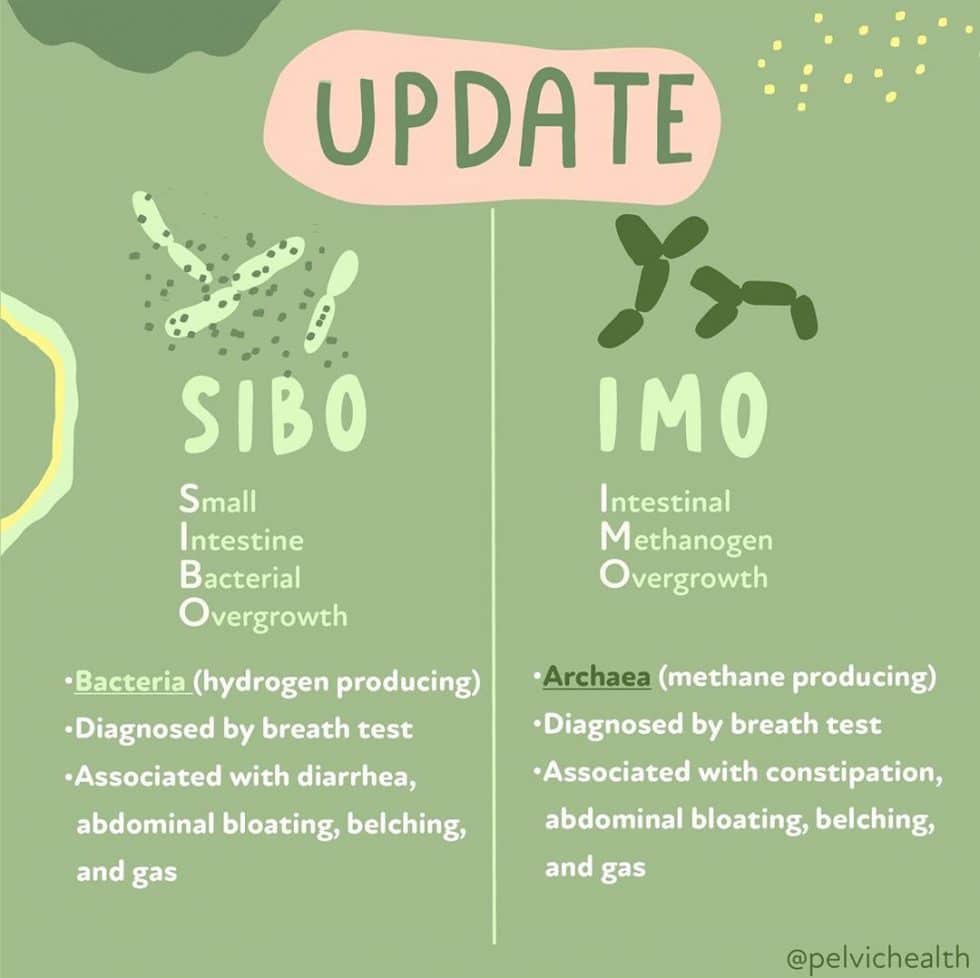
How to test for it:⠀
A breath test is typically used either in the clinic or a take-home test is given. The test uses a solution, glucose or lactulose (but usually lactulose), that is consumed and then one would blow into tubes at 20-30 min intervals which are then analyzed for the amount of hydrogen and methane gas that is expelled. If there is a specific amount of either gas at certain time points, the test is positive for overgrowth and there are a number of treatment options available. ⠀
⠀
Classic symptoms include:⠀
- Abdominal bloating 1-2 hrs after eating⠀
- Gas, belching, feeling of fullness
- Diarrhea and/or constipation⠀
- Brain fog
- Fatigue⠀
- Food sensitivities and reactions (if intestinal permeability occurs) ⠀
- Poor nutrient absorption (B12, iron)
These symptoms occur because the overgrown bacteria love certain types of fermented carbohydrates, known as FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols). The “low FODMAP diet” is a nutrition plan SIBO sufferers are regularly recommended to reduce their symptoms. ⠀
Did you know that people with pelvic pain syndromes (IC, endo) often also have SIBO and IMO?
⠀
Bowel Health⠀
Pelvic floor physical and occupational therapy can relieve constipation and improve continence by optimizing pelvic floor muscles function with manual therapy and exercise. If SIBO and IMO are present, treating the gut and the pelvic floor is necessary for improvement. ⠀
⠀
Endometriosis⠀
Women with endo are up to 5 times more likely to have gut dysbiosis and report symptoms such as “endo belly.” Surgery will not fix the gut dysbiosis but will allow treatment for SIBO and IMO to be more effective.⠀
⠀
Interstitial Cystitis/Painful Bladder Syndrome⠀
One study found 17 out of 21 patients with IC/PBS had a positive breath test for SIBO. SIBO and IMO often coexist with pelvic pain syndromes, we must test for and treat SIBO and IMO to improve outcomes.⠀
Q&A
Q: How is this diagnosed?
A: The most common test for SIBO is called a lactulose breath test. A physician can order the lactulose solution, which a patient drinks. The patient will then breathe into collection tubes 2-3 hours later.
Q: How long is Low FODMAP recommended for?
A: There is not a specific time frame, and it differs for everyone. Typically though, it is a therapeutic diet that should and should not be a “lifestyle” diet as it restricts many beneficial foods. It should also not be used to treat SIBO, but it can play a role in treatment when it is introduced at the appropriate time.
Q: How does the overgrowth even occur anyway?
A: Many reasons including chronic health conditions, stress, poor stomach acid (hypochlorhydria) and a big one is food poisoning, adhesions, slow motility.
Q: Is this the same as the H. Pylori test?
A: No, it is not the same as testing for H. Pylori.
Q: I was diagnosed with methane dominant SIBO 2 years ago finally – after years of digestive issues that would get worse the so called “healthier” I ate. I did not go the antibiotic round bc I can’t swallow large pills and the gastro said usually it’s 50/50 with success rate & high recurrence. I’ve been taking MegaSporeBiotic & putting it into food or drinks for the past 4 months & it def helps with some of my symptoms but I know I’m not absorbing nutrients properly bc of sibo – especially b12 which was on the much lower side of “normal” the last time I checked it 2 years ago. I get overwhelmed as hell with diet protocols – especially having IC & Vulvodynia too – I straight up panic at this point trying to come up with a game plan around food. A lot of people I’ve consulted with said it sounds like I have Candida too but I was only able to get the SIBO Test covered by insurance. I hear that a lot of people that have SIBO also have Vulvodynia & IC, is that accurate? Are there any supplements that help to support the clearance of SIBO in addition to diet? I just ordered a new multivitamin that I was told I can break open the capsule to take so hopefully I can get more of what I’m lacking!
A: Well, SIBO and IMO are often overlapping issues with pelvic health disorders when it comes to bowel health (constipation & diarrhea), endometriosis, and interstitial cystitis. This is the classic scenario of SIBO, most people only treat the overgrowth component but not the root cause and that is a common issue of recurrence. There are various supplements used to treat it at the root cause and some of them come in liquid form! This is the classic scenario of SIBO, most people only treat the overgrowth component but not the root cause and that is a common issue of recurrence. There are various supplements used to treat it at the root cause and some of them come in liquid form!
Q: Are prebiotics/probiotics or foods containing such helpful?
A: These are definitely important in addressing gut health and helping to ensure a good gut balance especially in preventing recurrence of SIBO, but need to be introduced at the right time. If introduced while SIBO is still present, this could further flare your symptoms. It is important to remember that SIBO is just an overgrowth of bacteria, not necessarily bad bacteria so introducing more bacteria (probiotics) or feeding all of it (prebiotics) may just make it worse.
Q: There is lots of information on how to detect and test it but not much on how to cure it. I have been on a low FODMAP diet for years and still have chronic bloating after eating. I don’t want to try the ‘rifaximin’ antibiotics as that is what I think caused my gut mess in the first place . Years of antibiotics as a teenager . So what are the cures for the bloating?
A: There is actually quite a bit of info on treatments, but treatment goes beyond treating just the overgrowth. That is often a “symptom” of something else. It is important to address both. The literature reports that antibiotic use is moderately effective and herbal therapy can be just as effective. IT is important to know which type of SIBO you have because it changes the course of treatment. As far as antibiotic therapy goes, not all antibiotic use is the same. For example, rifaximin is actually a more gentle one, whereas Cipro can wipe out the flora in one dose. But like I mentioned before, if you just treat the overgrowth but not the underlying cause, that is often the reason for failed treatment or recurrence.
Q: I think years of prescription meds have done this, is there anything natural I can do to help?
A: There are absolutely natural agents that can be effective for treatment! It is important to work with a provider though to know which ones are the right ones considering all that is going on and helping to also identify and treat the root cause.
Q: Hi, I recently found out I was highly positive for SIBO after dealing with issues with food for years and finally it escalated so badly I sought out help. I took the breath test and tested positive but I am methane predominant. I know sibo isn’t widely known so it’s been hard for me to find a GI that knows how to treat it. They put me on Cipro and that made things worse so I stopped. I follow a low FODMAP diet and even was before getting tested. Because I am methane predominant, is there a different way to go about treatment?
A: Yes, many conventional providers are not familiar, there are various antibiotics to treat SIBO and cipro is often not one of them and can have significant effects on the gut microbiome. There are natural approaches to treating all the types of SIBO. Although the low FODMAP diet can be used as a part of the treatment if it is used the right way, it is not a treatment for SIBO and caution should be taken for long-term use.
Q: I have thrush that I just cannot get rid of. It’s so painful. I am a vegan and don’t eat much refined sugar.
A: Thrush can be a symptom of gut issues, not necessarily SIBO. Certain diets can promote this and there can be other underlying causes other than just refined sugar. It is important to work with a healthcare provider that can help to figure out those underlying causes and help to treat it and address the underlying causes. Working with an integrative practitioner is ideal to work on both diet and can run functional tests and offer treatment options your conventional provider may not be able to do so.
Q: How is it treated with antibiotics?
A: There are a few different approaches, antibiotics are one and there are natural approaches like antimicrobials that can both be effective to treat SIBO.
______________________________________________________________________________________________________________________________________
Are you unable to come see us in person? We offer virtual physical and occupational therapy appointments too!
Due to COVID-19, we understand people may prefer to utilize our services from their homes. We also understand that many people do not have access to pelvic floor physical and occupational therapy and we are here to help! The Pelvic Health and Rehabilitation Center is a multi-city company of highly trained and specialized pelvic floor physical and occupational therapistss committed to helping people optimize their pelvic health and eliminate pelvic pain and dysfunction. We are here for you and ready to help, whether it is in-person or online.
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
In addition to virtual consultation with our physical and occupational therapistss, we also offer integrative health services with Jandra Mueller, DPT, MS. Jandra is a pelvic floor physical and occupational therapists who also has her Master’s degree in Integrative Health and Nutrition. She offers services such as hormone testing via the DUTCH test, comprehensive stool testing for gastrointestinal health concerns, and integrative health coaching and meal planning. For more information about her services and to schedule, please visit our Integrative Health website page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Like us on Facebook,
Subscribe to our YouTube Channel,
and follow us on Twitter, Instagram, Tik Tok and Pinterest!
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.