
Solving Female Sexual Dysfunction
By: Dr. Lisa Valle
What if the cure for adding more luster to your life is a fulfilling, sex life? But what happens when a woman feels distress about her sex life? Or she experiences sexual pain? Is there anything that she can do about it?
The answer is an emphatic yes!
There is an array of sexual conditions that can affect a woman’s sexual function. Female sexual dysfunction is defined as a perceived persistent problem with sexual response that causes her distress. This can include sexual pain, inability to achieve orgasm, arousal problems, and lack of sexual desire. This can be lifelong or acquired.
Unfortunately, many women are uncomfortable bringing this up with their physician. In addition, some physicians are uncomfortable addressing this issue as well. Finding a provider that is comfortable and skilled at evaluating and addressing these conditions is key to a successful treatment.
What is involved in an evaluation and treatment of female sexual dysfunction?
An in-depth medical history is first taken. We use this to seek out psychological, medical, and medication related causes of sexual dysfunction. This should also address relationship factors and satisfaction level, as well as socio-cultural attitudes. I feel that the most important part of the history is a focus on a detailed sexual history. This should include a focus on sexual activity, function, sexual/gender identity and orientation. An identification of the specific concern is made and a detailed assessment of how this affects her life and her level of distress is determined. In my practice, we use standardized questionnaires to help with the latter. This also gives us a baseline status to compare later on in her treatment.
In essence, an integrative, 360-degree approach to an evaluation is performed. A sexual problem is like a prism- each aspect of it needs to be addressed and treated. Examples of some topics that are often addressed might include: a history of trauma, attitudes and familial upbringing about sex, menopausal status, childbirth history, prior surgeries, medication and over the counter supplement usage. Throughout a woman’s life cycle, her feelings and needs about sexuality may change as may her relationships. Also, every woman’s sexual interest, response, and needs differ. The purpose of the history is to assess what specifically distresses her and how it is impacting her life and her relationships.
I believe that the most important factor to treatment of female sexual dysfunction is finding the correct diagnosis to address. In my practice, I take an integrative approach and explain to our patients that a team approach of utilizing other health professionals to help address her condition is key to a successful outcome. I first assess the patient’s goals and we address her expectations.
Firstly, any medical or psychological conditions that were discovered during her intake are addressed and the appropriate referrals are made. For example, if someone with sexual pain also has gastrointestinal complaints suggestive of irritable bowel syndrome or inflammatory bowel disease, I refer her to a gastroenterologist while we are treating her sexual condition.
Utilization of a network of sex therapists, marriage and family therapists, pelvic floor physical and occupational therapistss, neurologists specializing in treating pain, acupuncturists, nutritionists, gynecological dermatopathologists and others are vital to the management of her condition.
Lifestyle changes, nutrition and patient education regarding sexuality are also topics which are frequently discussed. Involving her partner with her treatment is also important.
Medications such as hormones, psychotropic agents, or herbal supplements are often used depending on the condition. If the sexual dysfunction is possibly related to the side effects of her medications, a discussion with the prescribing physician can be made to address this.
It is generally recommended that the patient be seen for regular follow up visits until her condition has improved.
What are risk factors of female sexual dysfunction?
As I mentioned previously, female sexual dysfunction has various facets to consider. The etiology can be from multiple issues such as: psychological (anxiety or depression), relationship issues, history of abuse, medication side effects (such as oral contraceptives), medical conditions (such as diabetes), fatigue, stress, and gynecological issues such as pelvic floor problems, endometriosis or a history of a traumatic delivery. Of note, this is not an all-inclusive list.
What are types of female sexual dysfunction?
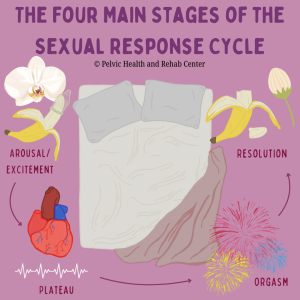
There are various phases in the sexual response cycle and each condition can frequently overlap. Female sexual dysfunction can be organized into the following general categories:
-Desire
-Arousal
-Orgasm
-Sexual pain disorders
Each category has specific conditions which cause distress for the patient. The listing and description of each diagnosis is beyond the scope of this particular blog post. To give an example, there are an array of sexual pain disorders such as: vulvodynia, vestibulodynia, pain related to endometriosis, overactive pelvic floor muscle dysfunction and pudendal neuralgia.
What does the physical exam involve?
Depending on the type of sexual concern, a targeted comprehensive gynecological exam is performed. A visual exam is performed making various observations of anatomy and structure. We look at any skin abnormalities. If pain is involved over the vestibule. which is the entryway of the vagina, a cotton swab or Q tip test is performed as well. The Q tip test involves very light touch along specific areas which are used to characterize the areas of tenderness using a numeric scale. Vulvoscopy is often used to exam skin changes that usually cannot be seen without magnification. Vulvoscopy involves a magnification lens and light which is used with diluted vinegar to look for precancerous skin changes or other dermatologic conditions. The abnormal areas often appear white. If this occurs, a small biopsy is recommended with a local anesthetic.
Testing for infections such as yeast, bacterial infections, sexual transmitted infections, and vaginal cultures can be obtained from a vaginal examination depending on the condition. An examination of the vaginal walls as well as the opening of the bladder should also be performed.
A muscular digital examination of the pelvic floor muscles as well as the nerve supply to the pelvic floor is utilized to assess for any areas of pain, tight muscles or tenderness.
What types of additional tests might be ordered?
As a gynecologist, we frequently order pelvic ultrasounds. I feel this is a great adjunct tool to the physical exam. A bimanual examination can frequently miss abnormalities. A CT scan or an MRI can sometimes be indicated as well. Hormonal testing via a blood test is routinely performed.
Overall, I feel that the time has come for women to embrace their sexuality and optimize their sexual health. It is an important facet to our humanity. Fortunately, more providers are learning how to evaluate and manage these conditions. It is my hope that female sexual dysfunction will no longer be a taboo topic but discussed openly and addressed appropriately.
About the guest author:
Lisa M. Valle, D.O., FACOG, ABIHM is a board certified Obstetrician/Gynecologist and has been in practice for over 12 years. Her integrative practice solely focuses on caring for women with female sexual concerns in Santa Monica, California. Her emphasis has been on concerns such as: pelvic & vulvovaginal pain disorders, loss/decreased libido, inability/difficulty achieving orgasm, arousal disorders, and various vulvovaginal disorders. She is a member of the International Society for the Study of Women’s Sexual Health (ISSWSH), the International Society for Sexual Medicine (ISSM), the Academy of Integrative Health & Medicine and a Fellow of the American College of Obstetricians & Gynecologists. Dr. Valle has been featured as a medical expert on TLC, the Discovery Health channel, radio, and print media. You can find her at her website at www.OWSFC.com or on Twitter, Facebook and Instagram at @Oasiswomensfc.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
I loved this article. I don’t think there is anyone in the Connecticut ,Rhode Island or Massachusetts area that would use this way of treating someone.
If there is, please let me know. I suffer from pudendul neurologia (?) and have had surgery. I’m divorced after many years without physical affection or sex. I was injured in 2008 and had decompression surgery in 2012.
I’m afraid to enter into a physical relationship in the future.
Hi Grace,
Please contact our Lexington, MA office at 781-862-5222.
Regards,
Admin