
By Guest Blogger Nicole Cozean, PT, DPT, WCS and author of The Interstitial Cystitis Solution
Pelvic floor physical and occupational therapy is the most proven treatment for interstitial cystitis. It’s the only therapy given an evidence grade of ‘A’ by the American Urological Association and recommended in the first line of medical treatment. But patients often wonder how does treating muscles and fascia reduce urinary symptoms and pain that seem to be coming from the bladder?
“Only a fraction of patients with the key symptoms of IC/BPS – urinary frequency, urgency, and pelvic pain – have ulcers within the bladder. And many of the patients who are diagnosed with IC/BPS are found not to have bladder pathology as the name implies, but rather pelvic floor dysfunction.”
– Dr. Kenneth Peters, Chair of Urology at Beaumont Hospital, MI
Goal of Pelvic Floor Physical and Occupational Therapy
The muscles of the pelvic floor are often tight in patients with IC, causing trigger points to develop in these muscles. When the body experiences pain, inflammation rushes to the site. Since IC is a chronic condition, the inflammation persists and begins to affect the fascia and muscles of the pelvis, inner thighs, and lower abdomen. Trigger points, muscle tightness, and inflammation can combine to irritate the nerves that run through the pelvis, which can cause pain to manifest throughout the pelvis and surrounding areas. The brain can also interpret these signals as the urgent need to go to the bathroom, which creates the urge to go even when you know the bladder is nearly empty.
We often refer to this as the dysfunction-inflammation-pain (DIP) cycle. The goal of physical and occupational therapy is to disrupt this feedback loop at every point we can. Releasing the trigger points in tight muscles can lessen pain and restore normal function to the pelvic muscles. Clearing inflammation that is present in the fascia (the thin layer between the skin and muscles underneath) can restore blood flow and reduce tender points. In turn, alleviating dysfunction and inflammation can reduce IC pain.
Pelvic Floor Dysfunction
One of the biggest myths of interstitial cystitis is that it is exclusively a bladder condition. Fewer than 10% of patients have confirmed damage to the lining of the bladder (known as Hunner’s lesions). In fact, experts in the field now believe the bladder to be an ‘innocent bystander’ in many cases of IC.
Some symptoms of IC can be caused by either the bladder or pelvic floor (or a combination of both). Others are exclusively due to the pelvic floor.
Bladder and/or Pelvic Floor Symptoms:
Bladder Pain
Urinary urgency/frequency
Nocturia (night-time urination)
Burning with urination
Suprapubic pain
Pelvic Floor Symptoms:
Low back pain
Pain with intercourse
Hip, groin, or tailbone pain
Difficulty starting/maintaining urine stream
Constipation
Even patients who have surgery to remove the bladder often still report the same symptoms persist after the procedure (which is now recommended only as a last resort).
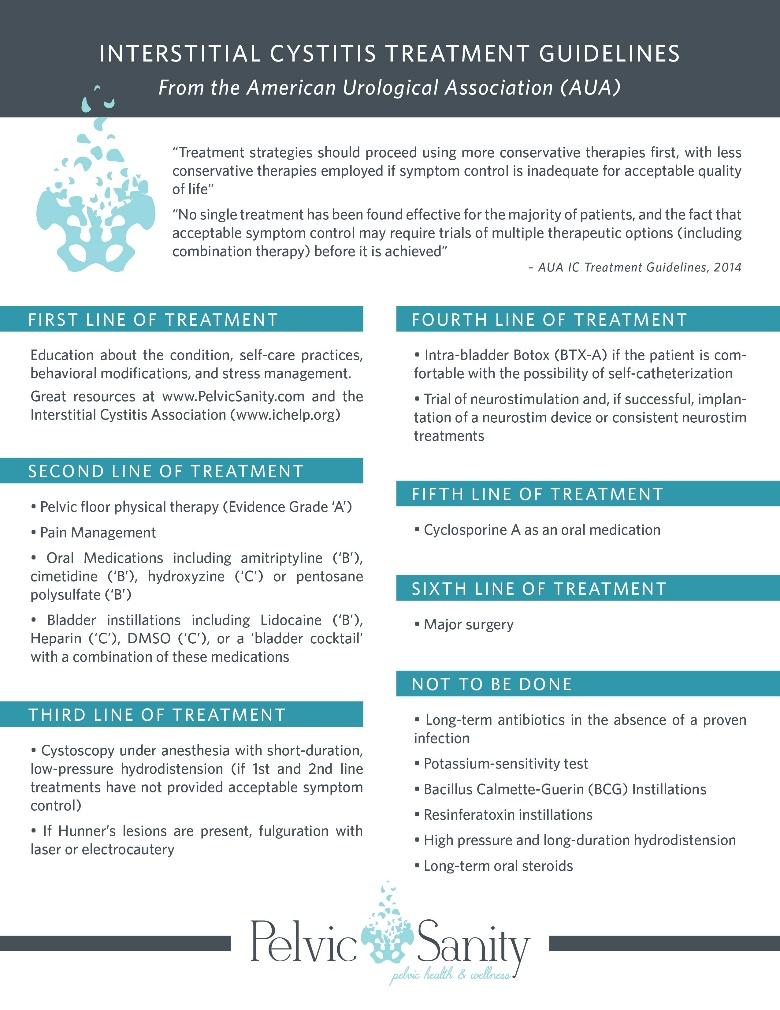
The American Urological Association IC Guidelines recommend physical and occupational therapy in the first line of medical treatment (2nd line overall), and physical and occupational therapy is the only treatment option given an ‘A’ evidence grade. Download the printable version here.
The Evidence for Physical and Occupational Therapy
Research into physical and occupational therapy for IC began almost 20 years ago, but many of the major findings have been published relatively recently. Two major, multi-center clinical trials conclusively established pelvic floor physical and occupational therapy as the most proven treatment option for IC in 2009 and 2012. Conducted by researchers from Stanford, Michigan University, the Cleveland Clinic, UPenn, and other prestigious programs, researchers found that nearly 90% of patients with IC experienced at least some improvement with manual physical and occupational therapy. Significant improvements in pain, urinary symptoms, and sexual dysfunction were all reported over the course of 10 one-hour sessions.
In a follow-up study conducted at our clinic and published by the International Pelvic Pain Society, patients reported more than a 65% improvement in IC pain and how much symptoms bothered them on a daily basis. More than half noted that they experienced benefits within the first three treatment sessions.

With all of this research, physical and occupational therapy remains the only treatment proven to sustainably benefit a majority of patients with interstitial cystitis.
What to Expect from Pelvic Floor Physical and Occupational Therapy
The goal of physical and occupational therapy with interstitial cystitis is the same as for more common conditions like knee or low back pain. We’re working to restore normal function to the muscles, prevent them from irritating nerves and causing pain, and clearing inflammation from the system. It’s just being performed in a more sensitive place, as some of the most important muscles can only be reached internally.
- Hour-Long Treatment Sessions. The studies in this area and most specialists conduct hour-long treatment sessions. This gives time to address the complexity of interstitial cystitis and to address both internal and external factors with each visit. If your pelvic PT only offers 30 minute sessions, you may consider trying to increase the frequency of visits or concentrate more on your home program to make up for the time.
- Both Internal and External PT. The pelvis is the crossroads of the body. It’s influenced by both the big external muscles that attach there (hamstrings, glutes, hip flexors, abdominals, and low back) as well as the smaller internal muscles of the pelvic floor. Your physical and occupational therapists should be finding and resolving issues in each of these muscles – we even spend a lot of time working on the calves of our patients, which are linked with the pelvis and often contribute to symptoms!
- Clearing Inflammation. The lower abdomen and inner thighs are both areas where inflammation tends to be present with IC. Clearing these areas is a high priority for patients in pelvic physical and occupational therapy.
- No Kegels. ‘Kegels’, or the voluntary squeeze and hold of the pelvic floor muscles (like you’re trying to hold back urine) should not be performed. These muscles are already overly tight; the goal of physical and occupational therapy is to relax these muscles, not further irritate and shorten them. Strengthening, including Kegels, may be appropriate later in treatment, after the pelvic floor is cleared and symptoms have been significantly reduced.
- No Pain. Physical therapy shouldn’t hurt or cause a pain flare. There may be some discomfort as we target trigger points and areas that are tender, but in general it should be tolerable. Symptoms may occasionally increase for a limited period, or you may be sore after treatment, but physical and occupational therapy shouldn’t increase your symptoms. Sometimes internal physical and occupational therapy is too painful when just starting out; in that case, your PT should focus externally until you’re able to tolerate internal treatment.
- Hands-On Treatment. Manual, hands-on therapy is the gold standard of IC treatment. There may be some benefit to biofeedback machines, but your treatment shouldn’t consist primarily of biofeedback. Just as IC is not just about the bladder, pelvic PT can’t be solely about the pelvic floor muscles – the entire pelvic and abdominal area needs to be addressed and treated.
Finding the Right PT for You
Research has shown that up to 70% of patients with IC have been to at least one (and often several) other physical and occupational therapistss before seeing a specialist in pelvic pain. There is a range of experience and knowledge among physical and occupational therapistss about the condition, so don’t assume that physical and occupational therapy doesn’t work after a single experience. You may need to try a different physical and occupational therapists (even at the same clinic). Don’t be afraid to ask about your physical and occupational therapists’s experience with the condition or seek a second opinion if you aren’t experiencing improvement.
We generally tell patients they should start to see a significant change – maybe not necessarily a wholesale improvement, but a definite difference – within the first 3-5 visits of physical and occupational therapy.
Self-Care Program
You should have a self-care program that is an extension of physical and occupational therapy, focused on maintaining and building on the gains of your physical and occupational therapy treatment. Seeing a physical and occupational therapists at their office for 1-2 hours a week isn’t enough by itself to make the lasting change that you need. The good news is that there is a lot that you can do on your own about the condition. Then, when you’ve reached your goals and are ready to be discharged, your home program will be your regular maintenance. Home exercises often include a combination of the following:
- Deep Breathing
- Stretching Regimen
- External Trigger Point Release (often with use of a foam roller)
- External Self-Massage (often focused on the fascia)
- Internal Trigger Point Release (often using a tool like the PelviWand®)
In Summary
Many of your IC symptoms may be coming from the pelvic floor – which is a good thing, because we can do something about them! Finding a qualified pelvic floor physical and occupational therapists can make a huge difference in your outcomes.
Realize physical and occupational therapy isn’t magic. It’s going to take dedicated work on your home program, and physical and occupational therapy should be one component of a multi-disciplinary approach that may also include medications, bladder treatments, eliminating trigger foods, and managing stress. But by combining external and internal physical and occupational therapy with a home program and medical management, patients can meet their goals, reduce their pain, and regain their lives.
Nicole Cozean, PT, DPT, WCS is a board-certified pelvic floor physical and occupational therapists and the author of the award-winning book The Interstitial Cystitis Solution. She was the first PT to serve on the Board of the Interstitial Cystitis Association and is teaching the first continuing education course for physical and occupational therapistss exclusively on IC in 2018 through the Herman & Wallace Institute. Nicole is the founder of PelvicSanity Physical and Occupational Therapy in Orange County, CA and treats patients from all over the world.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
I will always be grateful to my pelvic floor therapist. I got my life back after dealing with it for over twenty years. And I actually educated my urologist with what I learned to help the next male who might have these crazy and debilitating pains in an area that wasn’t well understood. Symptoms are to great for any noticeable cause was a favorite. Then the shrink gets ahold of the DSM and concocts some fancy disease and bam yer labeled.
I was diagnosed with IC almost 20 years ago. I’m one of the few that was afflicted with the Hunner ‘s ulcers. Through many surgeries, therapies, and medications, the ulcers have healed and now I’m left with the Pelvic Floor Dysfunction, which is more painful than anything I’ve experienced in the past. I’m currently seeing a new Physical Therapist and am hopeful things will get better. I’ll be printing this blog post off for her. Thank you for the good news!
THANK YOU, THANK YOU, THANK YOU. For far too long what physical therapy for IC should look like has seemed like a secret. I had to see the PT to find out what treatments they provided, and now I’m realizing there are many treatments that the therapists I’ve seen haven’t included. I hope more patients are able to get the treatments they should so we all can get better.
I will be starting therapy soon if the therapist approved. She took my information today about my symptoms and said she would get back to me. After reading this article I am more hopeful that it will help me. I have been in horrible pain for months and even pain medication does not stop pain from breaking through. I have almost given up hope what now after reading this I’m hopeful again. Thank you for all the great information