By Katie Hunter
I had the pleasure of attending Dr. Kenneth Peters’ lecture on the role of the Peripheral Nervous System(PNS) in the development and management of pelvic pain. Kenneth Peters, MD is a urologist practicing at Beaumont Hospital in Royal Oaks, MI, who specializes in treating complex pelvic pain including interstitial cystitis. For more information on Dr. Peters, check out his website here.
What is Interstitial Cystitis?
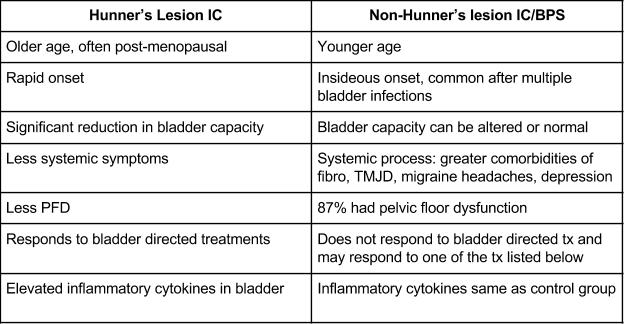
The first question Dr. Peters presents is how do we define “true” interstitial cystitis? Historically, the symptoms and diagnosis of interstitial cystitis have been classically defined by the presence of Hunner’s ulcers, most commonly seen in women, and described as pain in the bladder region at the anterior abdominal wall. In the 1943 Urology in General Practice textbook, there is a statement: “on behalf of women who complain of bladder trouble for which the average physician can find no cause, we plead that they not be condemned as neurotics until Hunner’s ulcers have been ruled out.” Fast forward to 1970 in the “bible of urology” textbook [according to Dr. Peters], Campbell’s Urology, where Hunner’s ulcers are described as “confusing, poorly understood, baffling etiology” that makes “a thoughtful physician wonder about the possibility of a mildly masochistic woman, i.e. destructive need in the female to suffer and ‘have trouble with’ her genitourinary apparatus.” Who wrote this textbook, Donald Trump? Dr. Peters’ point being, [much like our political climate today] while this was 30 years later, their thoughts were archaic and outdated. Luckily today, we have researchers and clinicians disproving these thoughts and validating this syndrome.
For more on the history of IC and current AUA Guidelines for the treatment of IC, check out Stephanie’s blog here.
“Hunner’s Lesion is a different disease and we should look at it as a separate entity,” according to Dr. Peters. Hunner’s lesion-IC and bladder pain syndrome or painful bladder syndrome are clearly distinguished in this lecture.
Dr. Peters quips that IC has been an oversimplified diagnosis and “if a patient hurts between their belly button and their knees, they’re told they have IC.” By giving a patient this diagnosis, a physician is defining their pain as a “bladder disease” which is misleading and results in inaccurate treatment plans and numerous failed treatments. This causes more fear in the patient that their symptoms will never resolve and often leads to distrust in the provider. Fortunately, through past, present, and future research, more and more providers will start recognizing the bladder as “an innocent bystander” in this population of patients.
I was very pleased that Dr. Peters emphasized that up to 87% of patients with the diagnosis of IC have pelvic floor dysfunction (PFD) and that PFD is likely an underlying cause or component of their symptoms. Even more exciting, he shares that he has received a significant Grant from the Department of Defense to study bladder directed therapy vs. pelvic floor directed therapy. We have already seen in past research that pelvic floor directed therapy was more successful in treating symptoms of IC than a general body massage (for more details about this study, check out Shannon’s blog here); but, it will be enlightening to many providers to see if pelvic floor directed therapy is more successful than bladder directed therapy. We hope his research will further emphasize the lack of efficacy for bladder directed treatments on non-Hunner’s lesion IC and reduce the number of failed treatments and procedures our patients must endure.
Non-Hunner’s lesion IC has overlapping symptoms with overactive bladder, pudendal neuralgia, vulvodynia, and CPPS. Patients with all of these diagnoses often have urinary urgency, frequency, and painful sex. Deferentially diagnosing the source of the symptoms will lead to successful outcomes.
Why do these various diagnoses have similar symptoms?
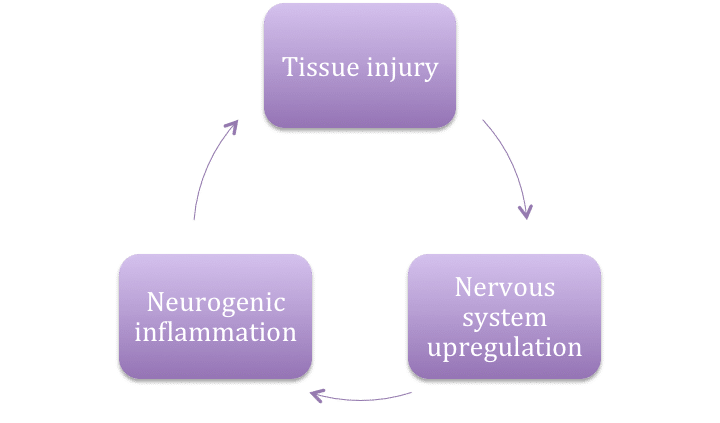
To answer this question, we must first understand what causes persisting pain. One theme of #WCAAP17 was the neurophysiology of chronic pain. Dr. Peters summarizes the whole picture of persisting pain in the following way:

Dr. Peters Image
Associated disorders of chronic pelvic pain include pelvic floor dysfunction, IC, prostatitis, IBS, urinary retention/incontinence, chronic constipation, headache disorders, fibromyalgia, and depression. As many of these disorders affect an organ, they may be defined as visceral pain syndromes in which pain arises in one or many organs. With visceral pain syndrome and CPP, we see an ongoing feedback loop of tissue injury, nervous system upregulation, and neurogenic inflammation. As pain persists in one organ, it may cause inflammation in the surrounding area, signalling a neighboring organ to elicit a painful response and the feedback loop continues. This is why it is essential for clinicians to assess and treat the “whole person” and explains why a multimodal treatment approach is required.
Dr. Peters Image
How do we treat this ongoing neuropathic feedback loop?
In developing a treatment plan, the biggest question is what is the driver of the pain? We are often thinking to ourselves, “which came first, the chicken or the egg?” because there are so many possible causes for these types of symptoms. For chronic pelvic pain and visceral pain syndromes, the most important nerve contributions are, in the periphery, the hypogastric, pelvic, and pudendal nerves; in the CNS, the right dorsomedial pons, periaqueduct, hypothalamus, and inferior frontal gyrus. The standard of care at this time is to treat all mechanisms of pain including both the peripheral and central nervous systems as this will successfully interrupt the ongoing feedback loop.
Treating the Peripheral Nervous System
At the periphery, activation of our c-fibers leads to our perception of pain in the brain. Repetitive activation of these fibers causes the response of the fibers to go up. My classic example is if you burn your hand on the stove and the next time you get close to the heat, your body reacts in a much bigger way by pulling away before you even touch the flame. This is partly due to the fibers in these nerves being more responsive – to protect us.
The pudendal nerve is one of the biggest players in pelvic pain, sexual pain disorder and IC – no surprise for us there! After the patient meets criteria of a pudendal neuralgia/neuropathy component which is currently defined by Nantes criteria, you can use focused treatments like diagnostic/therapeutic pudendal nerve blocks, pelvic floor physical and occupational therapy, electrotherapy, and neuromodulation. Electrotherapy can be used directly on a peripheral nerve that is suspected to be causing pain. This works to modulate impulses from the periphery and reduce pain signals to the brain. Neuromodulation can modulate impulses at all levels from the local nerve to the supraspinal level and cerebral cortex and “block” or “gate” the pain signal.
Treating the Central Nervous System
Due to a prolonged peripheral response to pain, our central nervous system starts to make changes and adaptations. This results in abnormal inhibitory reflexes, architectural changes in the spinal circuits and increased dendritic synapses, increased release of neurotransmitters, merging of the sensory and somatic nerve pathways, reduced filtration of sensory inputs, and an expansion of the sensory field. This explains why our patients with chronic pelvic pain will begin to feel pain when a non-painful stimulus is present; i.e. pain with touch, clothing, bladder filling, etc.
Neuromodulation is heavily supported by literature for treating chronic pelvic pain. While it affects the peripheral NS, it is also beneficial in treating these CNS adaptations. It does this by either re-balancing and normalizing our brain’s response or reducing the input to the brain. Neuromodulation may applied at either the sacral level (S3) of the spine or pudendal nerve which will affect S2, S3, and S4. This has been shown to reduce pain intensity and improve quality of life for patients with pelvic pain who did not have associated voiding dysfunction.
Alternative Pain Cycle
Dr. Peters also touches on an alternative pain cycle that many of our patients suffer from as their pain persists.

Dr. Peters Image
This picture is what we are often concerned with as physical and occupational therapistss. This emphasizes and supports the importance of addressing the muscles of the pelvic floor. Dr. Peters even states that these muscles should be treated first! By reducing muscle spasms and improving blood flow to the pelvis, this will help the treatments targeted towards the nervous system to be more effective and efficient.
Lastly, he emphasizes the need for a multidisciplinary approach, incorporating complementary therapies such as pelvic floor physical and occupational therapy, cognitive behavioral therapy, guided imagery, dietary modifications, and yoga/meditation to address all of the components of pelvic pain.
We thank Dr. Peters for a wonderful lecture and for sharing his clinical research that is helping so many of our patients! To view the Powerpoint in its entirety please start on page 107 here.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
Thank you! Always love to read what you write. It’s always positive and helpful.
The information you shared was very helpful. It explained a lot of the problems I have.
I am so glad I found this clinic and look forward to getting relief from this problem I have had for years
Dolores Rougeau
I have had pudendal nerve issues for over 5 years. I have tried physical therapy off and on for about 4 years plus or minus. Neither place i used was experinced with pudendal nerve in men. I did see a lady once in Chattanooga Tn. But the travel time was to much for frequent treatments. I initially went to see Dr Mark Conway in New Hampshire to confirm what i had. He did confirm my ONE. I have good improvement from initial onset over time, but still have issues. This article is the 1st time I have heard anything about Electrotherapy and Neuromodulation . Are you aware of anyone close to where I live that I could talk to? I live in North Alabama, Huntsville area.
Hello,
Please use the link below to find a pelvic floor physical therapist.
https://pelvicguru.com/2016/02/13/find-a-pelvic-health-professional/
Regards,
Admin
Tony,
Did you every find someone one to treat you i too am in Northeast Ala and would not mind going to Chattanooga if you could share the Dr names I would appreciate it so very much.
Thank you
Cindy
excellent issues you cover in this health article..