What is Chronic Prostatitis/Chronic Pelvic Pain Syndrome?
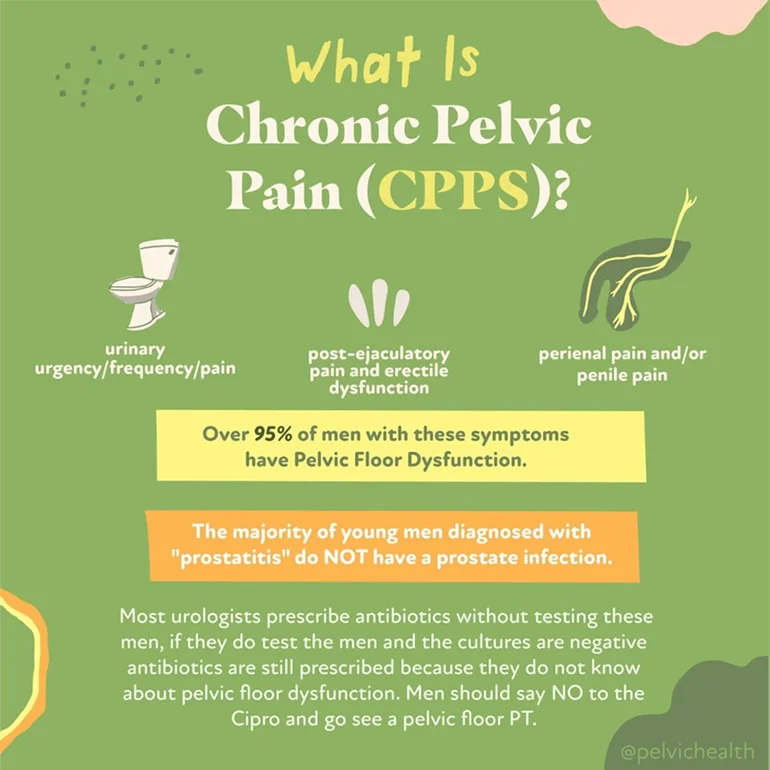
According to me (Stephanie Prendergast), these terms are outdated and not helpful for the management of the actual syndrome. The term “prostatitis” is misleading because roughly 97% of men with these symptoms do NOT have prostate pathology. The diagnosis “Chronic Pelvic Pain Syndrome” is problematic because the ‘chronic’ implies it will not resolve and ‘pelvic pain syndrome’ is nondescript and also useless.
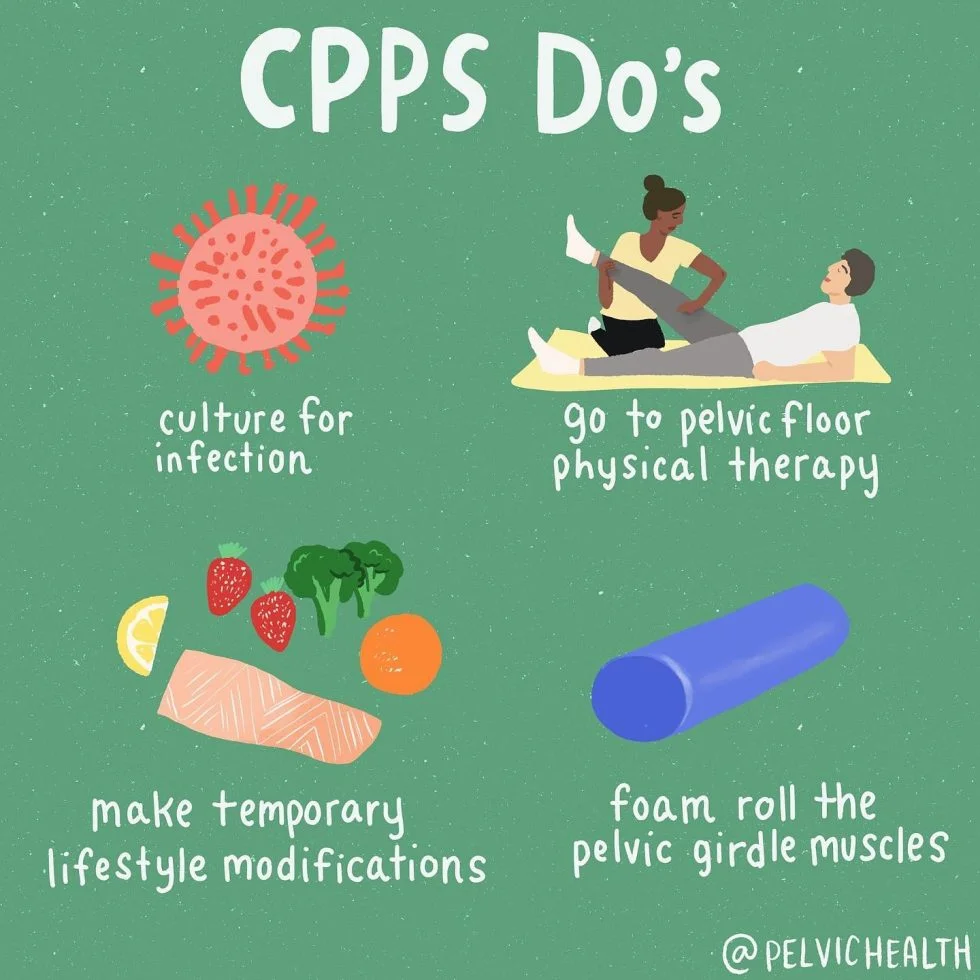
At the Pelvic Health and Rehabilitation Center we treat just as many male patients as women. This often surprises people, however, we have been trained to successfully treat men with pelvic pain syndromes. The majority of men suffering from CP/CPPS symptoms should always be referred to pelvic health therapy because studies show up to 90% of men have pelvic floor muscle and girdle dysfunction and the solution is pelvic floor physical and occupational therapy.
In addition to pelvic floor dysfunction, a few new studies came out recently showing additional therapeutic targets. We thought it would be fun to share these studies with you!
What’s New in CP/CPPS Research? A 2025 Update on Brain Biomarkers and Sexual Health
Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS) remains one of the most frustrating urologic conditions for patients and providers alike. Despite decades of research, its etiology remains elusive, its symptoms debilitating, and its treatments inconsistently effective. However, recent studies in 2025 have advanced our understanding of CP/CPPS in meaningful ways—especially in the realms of brain function and sexual health. In this blog post, we review two of the most recent peer-reviewed publications that shed light on the neurobiology and lived experience of those with CP/CPPS.
Understanding CP/CPPS
CP/CPPS is a chronic pain condition characterized by pelvic pain lasting at least 3 of the past 6 months, often associated with urinary symptoms, sexual dysfunction, and significant psychological distress. It accounts for up to 90–95% of all prostatitis diagnoses and disproportionately affects younger men in their reproductive years.
Because CP/CPPS does not have a clear infectious etiology, it is best conceptualized as a complex condition with multiple contributing factors—including muscular, neurological, psychosocial, and systemic components. The most promising research today seeks to uncover biomarkers and develop individualized treatment strategies based on a more nuanced understanding of the syndrome.
Brain-Based Biomarkers in CP/CPPS: A Groundbreaking Study
In one of the most exciting developments of 2025, a study published in Frontiers in Neuroscience used advanced neuroimaging to identify functional alterations in the brains of CP/CPPS patients. This study aimed to pinpoint objective biomarkers that correlate with symptom severity and to lay the groundwork for brain-based diagnostics and treatment monitoring.
Study Design & Methods
Researchers used two well-established imaging tools—Regional Homogeneity (ReHo) and Degree Centrality (DC)—to measure local brain activity and network connectivity, respectively. These scans were applied to a cohort of male CP/CPPS patients and compared with healthy controls.
Participants also completed the NIH Chronic Prostatitis Symptom Index (NIH-CPSI), which assesses pain, urinary symptoms, and quality of life. The researchers then analyzed how neuroimaging results correlated with the CPSI scores.
Key Findings
- Altered Connectivity in Key Regions: The study found significant changes in the right anterior cingulate cortex (ACC), amygdala, insula, and thalamus—regions all implicated in pain processing and emotional regulation.
- Degree Centrality (DC) as a Predictor: The DC value in the right ACC was especially noteworthy, showing a strong positive correlation with CPSI scores (r = 0.9654, p < 0.0001). This suggests that greater symptom severity is associated with altered connectivity in this brain region.
- Diagnostic Potential: With an Area Under the Curve (AUC) of 0.9654, the right ACC DC value demonstrated high potential as a biomarker for CP/CPPS.
Implications
This study provides further evidence that CP/CPPS is not simply a “pelvic” condition—it is a brain-body disorder involving altered central pain processing. These findings support the growing trend of incorporating central sensitization and pain neuroscience education into the clinical framework for managing CP/CPPS in addition to manual pelvic health physical and occupational therapy.
Additionally, this study lays the foundation for objective biomarkers that could help track treatment response or stratify patients based on their predominant pain mechanisms.
Citation:
Li, Q., et al. (2025). Altered Brain Functional Activity and Connectivity in Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A ReHo and Degree Centrality Study. Frontiers in Neuroscience, 19, 1511654. https://doi.org/10.3389/fnins.2025.1511654
Sexual Dysfunction in CP/CPPS: A Meta-Analysis
Another important contribution to the CP/CPPS literature in 2025 was a large-scale meta-analysis published in Medicina, which focused on the prevalence of sexual dysfunction among men with CP/CPPS. While previous research had hinted at these associations, this study provided more definitive estimates based on a large number of pooled studies.
Study Scope
The authors conducted a comprehensive review of 26 observational studies published between 2000 and January 2025. Databases searched included PubMed, Embase, Web of Science, and Google Scholar. Over 20,000 male participants with CP/CPPS were included in the final analysis.
Findings
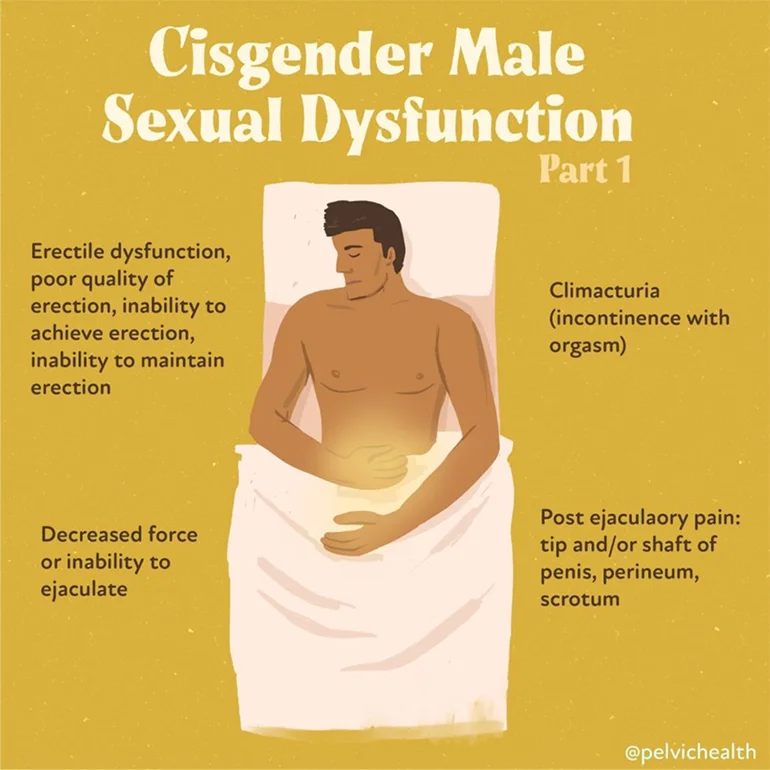
- Overall Sexual Dysfunction: 59% of men with CP/CPPS experienced some form of sexual dysfunction.
- Erectile Dysfunction (ED): 34% reported difficulty achieving or maintaining an erection.
- Premature Ejaculation (PE): 35% experienced PE
- Subgroup and Regional Variability: Prevalence rates varied significantly across studies, suggesting cultural, diagnostic, and healthcare access factors may influence reported rates.
Clinical Takeaways
Sexual dysfunction is not merely a secondary consequence of CP/CPPS—it is often a primary symptom. Erectile and ejaculatory dysfunction can significantly impact quality of life and may even precede the onset of pelvic pain in some cases. These findings highlight the need for multidisciplinary treatment, including pelvic floor physical and occupational therapy, psychosexual counseling, and urological management.
Furthermore, the high rates of dysfunction underscore the importance of proactive sexual health screening in this patient population. Many patients may feel ashamed or reluctant to report these symptoms unless specifically asked.
Citation:
Alibhai, M., et al. (2025). Sexual Dysfunction in Men with Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Systematic Review and Meta-Analysis. Medicina, 61(6), 1110. https://doi.org/10.3390/medicina6101110
What Do These Studies Mean for Patients and Providers?
Together, these two studies offer both hope and direction. The brain imaging findings validate what many patients already know—this condition is not “all in your head,” but it very much involves the brain. Pain processing is altered, and understanding that opens the door to new treatments including cognitive behavioral therapy, mindfulness, pain reprocessing therapy, and even neuromodulation.
At the same time, the high prevalence of sexual dysfunction calls for a broader view of CP/CPPS management. This is not a urological problem alone—it is a condition at the intersection of urology, pain science, sexual health, physical and occupational therapy, and mental health.
The Takeaway: It’s Time for a Holistic Framework
The era of prescribing antibiotics for every case of pelvic pain in men is over. The evidence now points us toward a biopsychosocial model—one that recognizes CP/CPPS as a chronic pain condition involving brain networks, pelvic floor dysfunction, and emotional factors. Both of the 2025 publications underscore the need for integrative care and patient-centered approaches that address the full spectrum of symptoms, including sexual health.
With objective biomarkers on the horizon and growing attention to quality-of-life concerns, the future of CP/CPPS research looks more promising than ever.
Let us help you!
The therapists at PHRC are highly trained to help men recover from pelvic pain and we want to help. Check out our website for more information, our reviews to see people just like yourself that have recovered, and a few additional resources we created.
Resources:
What to expect from an evaluation at PHRC
Male Pelvic Pain YouTube Resources
Interview with Stephanie Prendergast On the Hard Conversations Podcast
Frequently Asked Questions
What does it mean if I was diagnosed with chronic prostatitis, but my prostate is normal?
If you were told you have chronic prostatitis but testing shows your prostate is normal, you are not alone. About 97% of men who receive this diagnosis do not actually have a prostate infection or pathology. Instead, the symptoms often come from dysfunction in the pelvic floor muscles, tissues, and nerves. Tight or uncoordinated pelvic floor muscles can create pain, urinary changes, and sexual symptoms that mimic prostate problems.
Why is the term “chronic prostatitis” often misleading for men with pelvic pain?
The term “prostatitis” suggests the prostate is inflamed or infected, but research shows this is rarely the case. Most men labeled with prostatitis do not have bacteria or infection in the prostate. Using this term can actually delay proper care because men are often given antibiotics unnecessarily, rather than being referred to pelvic floor physical and occupational therapy, which addresses the real cause for most.
What is Chronic Pelvic Pain Syndrome, and why is this diagnosis not very helpful?
“Chronic Pelvic Pain Syndrome” is a very broad label that does not explain what is truly happening in the body. The word “chronic” can feel discouraging, as though symptoms will never improve. And “pelvic pain syndrome” is too vague to point to the actual source of the symptoms. As mentioned, the reality is that most men with this diagnosis have pelvic floor muscle dysfunction, which can be evaluated and treated with pelvic floor physical and occupational therapy.
If it’s not always the prostate, what causes the symptoms I’m experiencing?
For the vast majority of men, symptoms stem from the pelvic floor muscles and girdle. When these muscles become tense, irritated, or poorly coordinated, they can compress nerves, restrict blood flow, and create pain or urinary and sexual symptoms. Sometimes the spine or vascular system can also contribute, and conditions such as interstitial cystitis can overlap with these symptoms (as well as other conditions), which is why a thorough evaluation is so valuable.
Why should men with pelvic pain be referred to pelvic floor physical and occupational therapy?
Studies show that up to 90% of men with pelvic pain symptoms have pelvic floor muscle dysfunction. Pelvic floor physical and occupational therapy directly targets this dysfunction by calming irritated muscles, improving coordination, and restoring balance. Rather than treating chronic prostatitis symptoms with antibiotics for a suspected bacterial infection or using pain medications that don’t address the root issue, therapy focuses on resolving the muscular and nerve drivers of pain.
What role do pelvic floor muscles and the surrounding girdle play in male pelvic pain?
The pelvic floor muscles act like a hammock that supports the bladder, prostate gland, urethra, and rectum. When these muscles tighten or spasm, they can produce pain that feels like it’s coming from the prostate or bladder. Dysfunction in the pelvic girdle (including the hips, lower back, and core muscles) can further stress the pelvic floor, creating a cycle of tension and discomfort that looks similar to chronic nonbacterial prostatitis. In some cases, pelvic floor dysfunction can also mimic the symptoms of chronic prostatitis, prostate inflammation, or even prostate cancer, which is why a full evaluation is important. Physical and occupational therapy plays a significant role in identifying and addressing these muscle and girdle imbalances, breaking the cycle of pain, and restoring normal function.
What should I expect during a pelvic floor physical and occupational therapy evaluation?
During your evaluation at PHRC, our pelvic floor physical and occupational therapists review your full history, past diagnoses, and treatments you have tried. We listen carefully to your story because many men have gone through months or years of frustration before reaching us. The physical exam includes assessment of muscles, joints, nerves, and movement patterns, with special attention to the pelvic floor. At the end, we explain our findings clearly and create a treatment plan specific to your needs, often including both in-clinic therapy and a home program.
How long does it usually take to notice improvement with pelvic floor physical and occupational therapy?
Most men begin treatment one to two times per week for about 12 weeks. Many notice improvement within the first several sessions, though recovery can depend on how long symptoms have been present and whether other factors like spine or vascular issues are also contributing. With consistent therapy and home practice, it is possible to resolve symptoms over time.