
Ⓒ Redcord
By Sarah Court, PT, DPT, e-RYT
Traditionally, the thinking around how to approach low back and pelvic girdle pain has had a singular approach: find the ‘tight’ muscle and stretch it, and then find the ‘weak’ muscle and make it stronger.
While it’s true that muscular tone imbalances can and do create the kind of postural disequilibrium that leads to pain, in particular chronic pain syndromes, our approach needs to consider a broader perspective: how the brain is controlling the relative tone of our tissues, and how our muscles work together in what are called myofascial chains, or long links of muscles that are linked through fascial relationships.
Let’s look first at the myofascial relationships in the body. There are two different types of muscles in the body: global movers and local stabilizers. The global mover muscles are typically more on the surface of the body, and are made for creating movement – say, reaching for a glass, or doing a squat, or running up stairs. They are linked via their fascial relationships from head to toe, and work in conjunction with each other to create our movements. These muscles are made of fibers that can only sustain an output for a brief period of time – for the duration of the movement itself. Think of these like the sprinter muscles of your body: made to do a task that has a relatively short duration and a specific beginning and end.
What this can mean is if there is a weakness somewhere in the chain of linked muscles, it can lead to compensatory movement patterns and pain in a seemingly unrelated part of the body. For example, shoulder pain could be coming from a weak link in the hip, or a painful knee can be caused by a weak posterior line link on the opposite side of the body.
Local stabilizers, on the other hand, are deeper inside the body, and their job is to keep the torso stable while movement is taking place. Their fibers are made specifically for endurance, meaning their job is to be on at a lower level of engagement all the time that you are upright or moving around. These are your ‘marathon’ muscles: playing a supporting role throughout the day as you sit, stand, walk or run to provide stability to the trunk.
These local stabilizers have been identified as the diaphragm, the transversus abdominus, the multifidi, and the pelvic floor, and together they create a stable core for your body to move on top of.
When this muscle system isn’t working properly, it will often recruit some of the musculature of the global system as compensation, and since these ‘sprinter’ muscles burn out easily – muscles that aren’t even made to stabilize – it can lead to things like low back and pelvic pain.
So what might cause a disruption in this stabilizing system? In a word: trauma.
When an area of the body undergoes a painful experience, be it surgery, childbirth, a car accident, that experience is registered by the brain in a number of ways, and this creates a cascade of sensory and motor disruption.
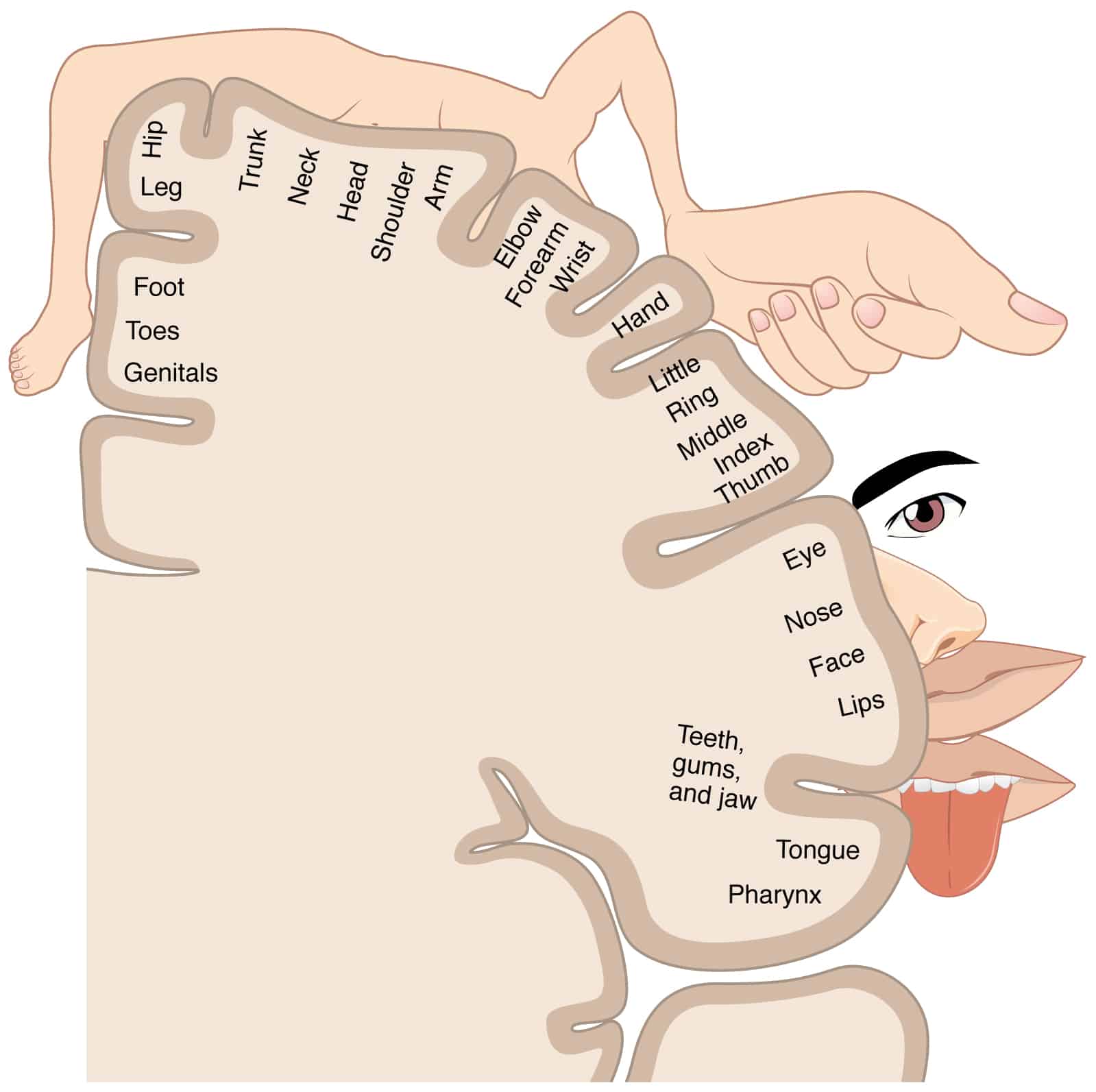
One of these effects is called cortical smudging.1 Your brain has two maps of your body that lie quite literally from ear to ear across the top of your head.
Schabrun SM, Elgueta-Cancino EL, Hodges PW. Smudging of the Motor Cortex is Related to the Severity of Low Back Pain. Spine 2017 Aug 1;42(15):1172-1178.
There’s a version for sensation, and a version for movement, and they are side by side on the top of your brain where the sensory and motor cortices meet. When pain is experienced in a certain part of the body, it affects these two maps by ‘smudging’ that area of the map. For the sensory map, if pain is chronic and ongoing, this smudge makes it difficult for the brain to figure out the exact location of the pain (which is why it can feel like it moves around, or it’s in a general area, but hard to pinpoint).
For the motor map, the smudging makes it very difficult for the brain to send movement messages to that part of the body. So in the instance of pelvic floor trauma, when the neuromuscular communication to the local stabilizers has been disrupted, the brain creates a compensatory movement pattern using different muscles, such as the paraspinals of the low back, which in turn become overworked, exhausted, and ultimately painful.
Simply stretching or massaging the low back won’t sufficiently address the problem. We have to reset the brain’s communication with these areas of the body, via a technique called neuromuscular activation, which is one of the techniques we use at Postureworks.
With neuromuscular activation, we stimulate the correct muscles to come on at the right time. For the local stabilizers of the core, which includes the pelvic floor, we use suspension and high frequency vibration to re-activate these stabilizers without pain or compensation. Retraining the neuromuscular system takes frequent repetition, as we are quite literally re-mapping the brain’s connection to this part of the body for proper activation. With repetition, correcting these imbalances via resetting the neuromuscular control will train the brain to stop using the wrong muscles for the job and thus get rid of painful dysfunctional patterns.
To find a Red Cord provider in your area please visit www.redcordamerica.com .
Links to Posture Works in Los Angeles:
About Sarah:

Sarah Court, PT, DPT, e-RYT graduated with a Doctor in Physical and Occupational Therapy from Mount St. Mary’s University. She has experience in orthopedic and neurologic settings, rehabilitating patients post-surgery or injury, and managing chronic neuromuscular conditions. Since 2005, Sarah has been an international yoga teacher and yoga teacher trainer, and developed her own continuing education program for movement professionals. She gives clients the tools to move intelligently, and integrates Neurac/Redcord, yoga, and other movement and breathing techniques into her treatments. Sarah has a BA in Art and Architecture from Princeton University.
References:
- Schabrun SM, Elgueta-Cancino EL, Hodges PW. Smudging of the Motor Cortex is Related to the Severity of Low Back Pain. Spine 2017 Aug 1;42(15):1172-1178.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.