What’s new in research and clinical care for “Prostatitis” aka male Chronic Pelvic Pain Syndrome (CPPS)?
By Stephanie Prendergast, Cofounder, PHRC Los Angeles
If you are a man suffering from what feels like ‘prostatitis’, this blog and our upcoming informational event is for you.
Did you know?…
- 10% of men experience prostatitis-like symptoms at some point in their lives.
- 97% of these men do not have a prostate or bladder infection yet are still treated with antibiotics.
- The majority of these men have pelvic floor dysfunction and can benefit from pelvic floor physical therapy.
Since the early 2000’s research has consistently shown the prostate itself is not the problem nor is the prostate infected. Unfortunately here in 2018 there is continued misuse of the prostatitis diagnosis and subsequent medical mismanagement of suffering men.
Medical professionals specializing in urologic male pelvic pain, otherwise known as Chronic Pelvic Pain Syndrome (CPPS) want to change that. Jason Kutch, PhD organized a free event for men with CPPS at USC in Los Angeles on Wednesday, May 9, 2018 from 6:00 – 8:00pm. If you do not live in Los Angeles do not worry, the medical panel will be filmed and distributed.

Symptoms
Symptoms of CPPS can include some, all or a combination of the following symptoms:
- Difficulty urinating, starting the urinary stream, or straining to urinate
- Urinary urgency and frequency
- Burning during or after urination
- Changes in erectile quality, strength of ejaculate and/or orgasm intensity
- Pain with ejaculation
- Pain and/or difficulty with bowel movement
- Perineal, penile or anal pain
- Perineal, penile or anal pain with sitting and/or exercise
- Pain within the perineum region during sitting
Terminology
Over the past two decades there has been increasing evidence that multiple factors other than prostate and bladder dysfunction cause CPPS symptoms. As a result there has been debate about what urologic pelvic pain syndromes are and should be called. These terms include:
- National Institute of Health categorization of Prostatitis
- Category I: Acute systemic infection of prostate or bladder
- Category II: Chronic bacterial prostatitis (CBP) which is caused by chronic bacterial infection of the prostate with or without prostatitis symptoms and usually with recurrent UTIs caused by the same bacterial strain.
- Category III: Chronic prostatitis/chronic pelvic pain syndrome which is characterized by chronic pelvic pain symptoms and possibly voiding symptoms in the absence of UTI.
- Category IIIa: Category III CPPS with the presence of inflammatory cells in prostatic secretions
- Category IIIb: Category III CPPS without inflammatory cells in prostatic secretion
- Category IV: Asymptomatic inflammatory prostatitis (AIP) which is characterized by prostate inflammation in the absence of genitourinary tract symptoms.
- NIH categories III, IIIa, and IIIb are the most similar to CPPS because there is not active infection. Other terms include:
- Nonbacterial Chronic Prostatitis
- Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS)
- Interstitial Cystitis/Painful Bladder Syndrome (IC/PBS)
- Male Pelvic Pain Syndrome (MPPS)
For the sake of this post we call the syndrome Chronic Pelvic Pain Syndrome (CPPS).
If it’s not a prostate infection, what is it?
CPPS is considered a heterogeneous syndrome, meaning it can have multiple and sometimes overlapping causes. CPPS is not a disease and therefore the underlying causes will vary from individual to individual. However, new studies are pointing to pelvic floor muscles as a major contributor to CPPS symptoms.
Diagnosis and Treatment
Because of the variability in each individual’s case diagnosis and treatment needs to be individualized.
On May 9th, 4 expert medical professionals will explain the latest advances in diagnosing and treating CPPS. The panel has been organized by researcher and neuroscientist Dr. Jason Kutch, and is interdisciplinary to reflect the different areas of involvement of CPPS.
The Panel

Dr. Kutch will discuss research efforts by the National Institutes of Health (NIH) to create a new understanding of CPPS that will improve treatment. Urologist Dr. Joshua Gonzalez will talk about the proper medical evaluation and treatment for men with CPPS. Pelvic floor physical and occupational therapistss Daniel Kirages and Stephanie Prendergast will discuss the role the pelvic floor muscles and musculoskeletal system play in in CPPS. Finally, the panel will discuss effective treatment options and where men across America can find appropriate providers to help them. This event is open to patients, their families, and medical providers interested in the topic.
Event Details
Wednesday, May 9, 2018 6pm-8pm
1540 E. Alcazar St, Los Angeles, CA 90033
Parking available. Please RSVP to Jason Kutch (kutch@usc.edu) by Wednesday May 2, 2018.
Thank-you and we hope to see you there!
FAQ
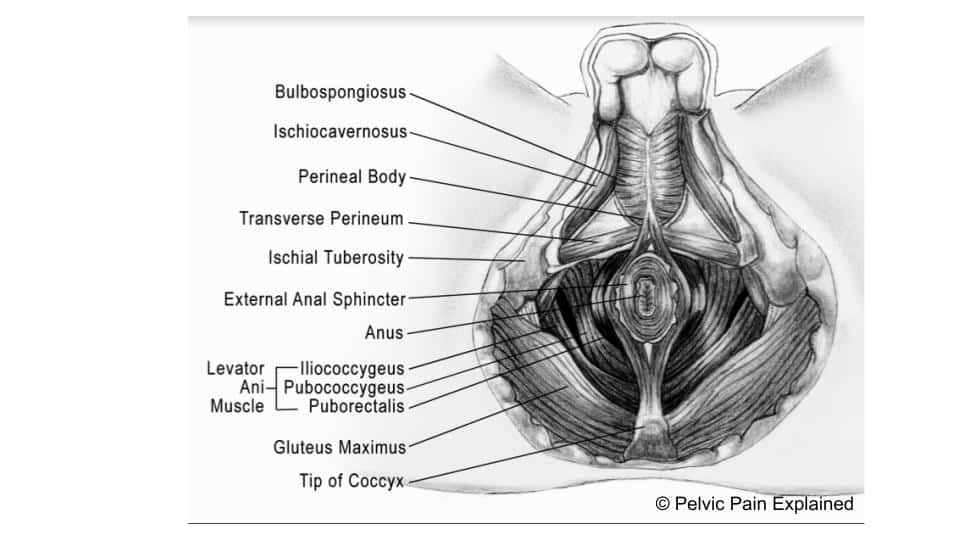
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
My daughter Colleen guest is a physical therapist specializes in pelvic floor. She forwarded this information to me. I like to be any memory of us thank you
Very interested to share with my patients after it is filmed and available since we are out in Seattle and cannot make to the actual event.
How can we /they access the Class after recording?
thanks and Bravo for doing and putting out there!
Hi Kathy,
The video is on PHRC’s Facebook page.
Regards,
Admin
It said this will be filmed…. is this available on the web?
Hi Ben,
Yes! It is on PHRC’s Facebook page.