
By: Rachel Daof, DPT
Los Angeles PHRC members, Stephanie Prendergast, Courtney Edgecomb, and I, Rachel Daof, went to a dinner to discuss Intrarosa with guest speaker Dr. Irwin Goldstein. One of the major points of the night was this: menopause is a chronic progressive, degenerative condition, and it does not improve without treatment. This hit home to all of the women in the room because we all were, are, or are going to experience this milestone in life. Menopause is when a woman does not have a period for 12 consecutive months by the depletion of ovarian follicles/oocytes.1 Consequently, women will have a significant decrease in reproductive hormones, which is essential to keeping the genitourinary area healthy and symptom free. The conversation progressed to what the genitourinary region would look like once a woman has gone through menopause. It was answered: genitourinary syndrome of menopause (GSM) would occur.
1. What is GSM?2
GSM affects the labia majora and minora, vestibule (vaginal entrance), clitoris, vagina, urethra, and bladder. As reported by Simon, the changes include a “[reduction] in collagen and elastin, thinning of epithelium, altered function of smooth muscle, loss of elasticity and flexibility, and diminished blood supply” to the above regions. As a result, the signs and symptoms of GSM include, but are not limited to, the following:
- “irritation, burning, and itching of the introitus
- dysuria, urinary frequency, and urgency, recurrent urinary tract infections
- vaginal dryness, fissures at the posterior fourchette, labial resoption, pallor/erythema, loss of vaginal rugae, protrusion of the urethral meatus and urethral sensitivity, and also sexual symptoms of diminished lubrication, vaginal, vestibular or vulvar discomfort or pain with sex, or impaired sexual function (desire, arousal, orgasm).”2
2. Genitourinary structures require both estrogen and androgens
The first thing you should know about genitourinary health regarding this topic is that the ovaries and the adrenal glands are the main suppliers of female sex hormones. It is important to note that all androgen sex steroid hormones are as important as mere estrogen to maintain genitourinary health. These androgens include: “DHEA, androstenedione, androstenediol, testosterone, and 5α-dihydrotestosterone (5α-DHT), . . . [and] androgen receptors are widespread throughout the genitourinary tract (clitoris, vestibule, urethra, bladder, vagina, female prostate tissue).”2 Premenopausal women produce a significantly greater amount of androgens than estrogen alone, and androgens are able to biosynthesize into estrogens. View the following chart for more detailed information:
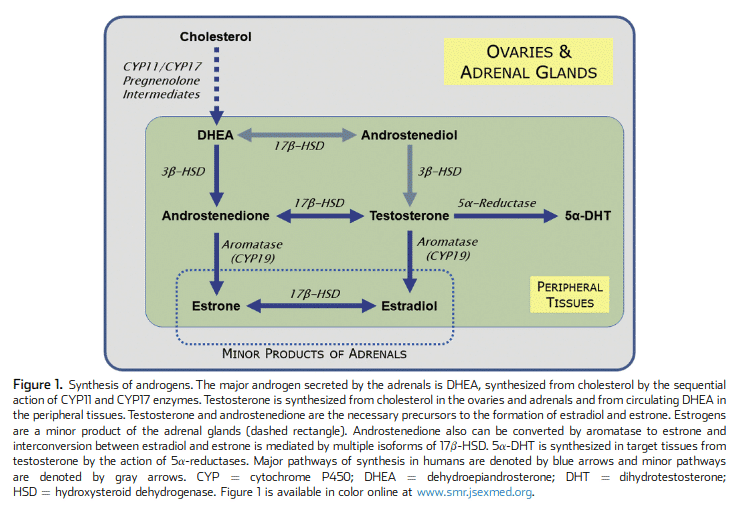
(Traish)3
As you can see in the chart above, DHEA is the main androgen secreted by the adrenal glands to then synthesize other sex hormones. At about 30 years old, your body starts to have a natural decline of DHEA; however, it is still available. The thing about menopause is that you don’t get these much needed hormones from your ovaries anymore, and you rely solely on DHEA, which has already declined about 60%. Therefore, signs and symptoms of androgen and estrogen decline will parallel the decline of DHEA because it is the main source that is left supplying the vulvovaginal region of necessary hormones.2 To beat a dead horse, you need androgens for genitourinary health.
Circling back to menopause, the genitourinary system is greatly impacted when there is a decrease in estrogen and androgens. Many women are currently using just estrogen to combat menopausal symptoms, but we now know that doesn’t suffice. Prior to 1942, it was commonplace to be treated with ovarian extracts which contain both estrogen and androgens. It is time we start looking at both estrogen and androgens again to combat GSM.
3. Diagnosis of GSM2
If you suspect that you have GSM, it is time to go to a skilled health care professional to confirm a diagnosis. Confirmation will include:
- Vaginal pH >/= 5.0: A healthy pH ranges from 3.5 – 5.0. Above 5.0 is indicative of vaginal atrophy due to hormonal deficiency.
- Decreased content of superficial cells and increased proportion of parabasal cells: This is confirmed with microscopic evaluation of a vaginal smear.
- Serum hormone levels (when necessary): “Although the components of GSM are a consequence of sex steroid deficiency, no laboratory blood tests will either confirm or negate the diagnosis, because there is no cut-off serum concentration for any sex steroid below which most women will experience symptoms of GSM. Some women experience substantial symptoms of GSM even when they are using systemic hormone therapy (particularly the lower doses currently recommended for oral therapies), and may require concurrent local treatment, while other women may be asymptomatic with very low serum sex steroid levels.”2
4. Treatment of GSM
Intravaginal DHEA (prasterone, the active ingredient in Intrarosa) has been approved by the FDA for the management of moderate to severe dyspareunia due to menopause. After intravaginal DHEA is placed, it is then converted by enzymes within the vagina via intracrine metabolism to then produce estrogens and androgens (androstenediol, androstenedione, testosterone, and DHT). This means that the DHEA that is placed intravaginally will not be taken up systemically, and it stays within the genitourinary region. DHEA is inactive until it is “transformed inside the cells into cell-specific amounts of estrogens and androgens.” This means, only “inactive metabolites” are in circulation which “eliminates the risk of an influence in other tissues. This treats the tissues locally while having the rest of the body maintain normal levels of sex steroids. “DHEA only replaces what is missing at the right place and in the right amount.”2 It stays inactive in your system until your body needs it, so you do not go over normal levels of DHEA. What it is mainly prescribed for is pain for postmenopausal women, and it is a vaginal insert. If you are experiencing pain with intercourse after menopause, please visit Intrarosa’s website here and talk to your medical provider for a prescription.
Compounded topical estrogen and testosterone has also been used for vestibulodynia in premenopausal women with great success, but there is lacking research with postmenopausal women. For more information on premenopausal vestibulodynia and oral contraceptives, please look into this blog (and part two) written by Dr. Joshua Gonzalez.
The symptoms women experience in menopause such as painful sex, urinary urgency/frequency, and vulvar pain are also symptoms of pelvic floor dysfunction. If you are experiencing these symptoms a combination of medical management and pelvic floor physical and occupational therapy can help! Check out our website and our book, Pelvic Pain Explained, for more information.
References:
- Menopause. UCLA Obstetrics and Gynecology. http://obgyn.ucla.edu/menopause. Accessed August 13, 2019.
- Simon JA, Goldstein I, Kim NN, et al. The role of androgens in the treatment of genitourinary syndrome of menopause (GSM). Menopause. 2018;25(7):837-847. doi:10.1097/gme.0000000000001138.
- Traish AM, Vignozzi L, Simon JA, Goldstein I, Kim NN. Role of Androgens in Female Genitourinary Tissue Structure and Function: Implications in the Genitourinary Syndrome of Menopause. Sexual Medicine Reviews. 2018;6(4):558-571. doi:10.1016/j.sxmr.2018.03.005.
- Labrie F. Intracrinology and menopause. Menopause. 2019;26(2):220-224. doi:10.1097/gme.0000000000001177.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.