By Stephanie A. Prendergast, MPT, Cofounder, PHRC Los Angeles
Why do my sitz bones hurt with sitting, but not when sitting on the toilet?
Alexandria’s Success Story with Highs and Lows throughout the Healing Process
The History of Alexandria’s Pain and How She Found PHRC
Alexandria is a 62-year-old female who showed up to PHRC with eight out of ten searing, shooting pain starting in her left sitz bone traveling down into her peri-vaginal and peri-rectal areas that was aggravated by sitting and driving for longer than five minutes, bending forward to pick up cat litter from the ground, riding her recumbent bike for longer than three minutes, and gardening. Her symptoms were eased by walking, lying down, standing, and sitting on the toilet seat. She denied noticing any correlation between her symptoms and urinary, bowel, or sexual activities. Her symptoms started insidiously in 2016, which is when her orthopedic doctor referred her to a chiropractor and to orthopedic physical and occupational therapy. However, she reported that the hip and core strengthening exercises she did for six to eight weeks with her orthopedic physical and occupational therapists did not improve her symptoms. Since her symptoms persisted, she reached out to her OBGYN and nurse practitioner about one year ago, who mentioned that they were not familiar with her symptoms and referred her to PHRC for pelvic floor therapy. She also has a history of a spinal fusion in 1981 due to scoliosis, a right knee arthroscopy in 2016 due to arthritic changes, and arthritic pain in the joints of her hands. For several months before our first visit together, she had been working with a personal trainer at the gym to lift heavy weights (up to ~300 lbs.) and build leg strength by using the leg press. More recently and through the course of our treatment sessions, she also started to report pain and clicking in her right hip when walking or stepping up/down curbs.
Physical Exam and Assessment
During her initial evaluation, I noted the following findings:
- Proper lumbopelvic mechanics with spinal flexion to pick object off ground, but noted increased bias and weight bearing through right leg vs. left
- Moderate connective tissue dysfunction along her abdomen, inner thighs, suprapubic region, and bony pelvis
- Myofascial trigger points along the psoas major, adductors, glutes, and hip external rotators, specifically obturator internus and piriformis
- Fascial restrictions and decreased connective tissue/neural mobility along the dorsal branch and inferior rectal branch of the pudendal nerve as she reported tenderness only on the left side
- Hypertonicity (tightness) throughout the urogenital diaphragm (specifically ischiocavernosus and superficial transverse perineal muscles), obturator internus, and levator ani, which were all tender to touch only on the left side
- Decreased pelvic floor range of motion along with poor ability to lengthen and relax the pelvic floor muscles voluntarily
- Positive Tinel’s sign at left Alcock’s canal and along the left dorsal branch of the pudendal nerve as she reported increased burning sensation with palpation of these areas
My assessment was that Alexandria was experiencing symptoms of left-sided pudendal neuralgia secondary to connective tissue/fascial restrictions along her bony pelvis, increased hypertonicity throughout her pelvic floor as well as altered movement mechanics throughout her activities of daily living due to her history of the spinal fusion, right knee arthroscopy in 2016, and arthritic changes in her other joints. During the internal assessment on our first day, she reported a “burning and dry” sensation with palpation of all the pelvic floor muscles on the left side, especially along the urogenital diaphragm and obturator internus, but denied reproduction of these sensations on the right side of the pelvis. In addition, she presented with the most amount of tension at her left obturator internus and reported a burning sensation when I tapped along different branches of her pudendal nerve, which is indicative of a positive Tinel’s sign.
This makes sense when you think about her objective findings in relation to her symptoms. Pudendal neuralgia generally presents as burning, shooting, stabbing pain, and possibly altered sensation/numbness in the nerve distribution. The pudendal nerve divides into three branches, including the dorsal clitoral/penile branch, perineal branch, and inferior rectal branch. It supplies sensory information and controls the pelvic floor muscles through motor fibers. The sensory fibers supply the sensation to the clitoris, parts of the vulva, lower labia, perineum, and anal canal in females and to the penis, posterior scrotum, perineum, and anal canal in males. Motor functions of the nerve include urinary/fecal continence, urination, evacuation of stool, clitoral/penile erections, and orgasm/ejaculation. Causes of nerve injury or irritation may include compression (e.g. prolonged sitting, bicycling, horseback riding), tension (e.g. chronic constipation, straining, squatting, childbirth, biomechanical dysfunction), infectious (e.g. repetitive yeast infections, dermatologic triggers), surgical insult, or insidious. Visit this blog to read more about pudendal nerve anatomy and how bicycling can affect the pelvic floor muscles.
Alexandria symptoms are one-sided and she specifically reports “searing, shooting, and burning” pain only on her left side. Her symptoms are aggravated by sitting, driving, and recumbent bicycling, which are all compressive forces on the nerve, and by forward bending and using the leg press, which are tension forces on the nerve. She presented with connective tissue restrictions along all three branches of the nerve during the external exam and presented with myofascial trigger points and hypertonus throughout the left side of her pelvic floor, which are further contributing factors to her symptoms since tight fascia and muscles can compress on the nerve and irritate it. Neuralgia and hypertonic muscles often exist together as tight muscles can cause nerve irritation, but nerve pain can also cause muscle tension as it may be the body’s reaction to guard against the pain. In addition, it is possible that she started to unconsciously alter her biomechanics after her right knee arthroscopy procedure in 2016 and compensate with her left leg during activities like sitting, walking, and gardening, which could have led to changes in the mobility of her joints and ligaments in her pelvis as well as overuse of her left pelvic floor muscles. She did specify that the arthroscopy actually made her knee pain worse afterwards. Overall, these could all be possible contributors to Alexandria’s symptoms.
My Plan and Goals for Alexandria
Alexandria’s goals were the following:
- Alleviate symptoms to return to reading in a seated position without pain
- Alleviate symptoms to pick up cat litter off the ground with less pain
Based on Alexandria’s symptom description, objective findings, and orthopedic history, it was clear to me that the cause of Alexandria’s symptoms was biomechanical and musculoskeletal, leading to nerve pain. My plan for her was physical and occupational therapy one time a week for the next eight to twelve visits as nerve-related pain generally requires a longer healing process due to the slow nature of nerve regeneration (~one mm/day). In order to monitor her progress in every visit, I set both short-term and long-term goals for Alexandria.
My short-term goals were:
- Patient will normalize connective tissue mobility to improve blood flow and tissue function.
- Patient will demonstrate good motor control for pelvic floor drop to improve pelvic floor tone.
My long-term goals were:
- Patient will be able to pick up cat litter off the ground without pain.
- Patient will be able to sit to read/watch TV and drive for >one hour without pain.
- Patient will be able to use her recumbent bike for 10 minutes/day without pain.
During her initial evaluation, we discussed how chronic pain can affect the nervous system as well as how her intense exercise regime with her personal trainer could play a role in exacerbating her symptoms. I suggested she probably has to either limit or completely cease her sessions with her personal trainer since performing the leg press loaded with 300 pounds could really aggravate her symptoms. I also educated her about how neuropathic pain can have a delayed onset (e.g. feeling pain-free while doing 30 reps of heavy weight squatting, but feeling increased pain 40 minutes later), so she should be mindful about how long she is riding her recumbent bike for now. Furthermore, we talked about different options for seat cushions that function to offload pressure off of the perineal and anal area, so sitting and driving can be more manageable for her while she is recovering. Diaphragmatic breathing exercises were given as the first part of her home exercise program to address restrictions in her pelvic floor and to stimulate her parasympathetic nervous system.
My plan for future treatment sessions involved connective tissue manipulation, myofascial release, myofascial trigger point release, neuromuscular reeducation, nerve glides, therapeutic exercise and activity, and home exercise program prescription and management. There was going to be an emphasis on improving the range of her pelvic floor by teaching her how to voluntarily lengthen the muscles through doing pelvic floor drops. In addition, my plan included progressing her to a point where she can independently perform nerve glides, which include mobilizing the nerve to improve blood flow and oxygen to the nerve itself as well as the surrounding muscles, at home within a pain-free range.
The Course of Alexandria’s Recovery
At Alexandria’s first follow-up visit, she reported that her pain has been less frequent and less severe after being consistent with the breathing exercises. She also heeded my advice by discontinuing her sessions with the personal trainer. Throughout the course of all our visits, we worked on improving connective tissue mobility and addressing myofascial impairments, such as trigger points present in her abdomen, adductors, bony pelvis, glutes, and low back, with the use of cupping. More information about the causes and treatment for connective tissue restrictions and for an explanation of cupping techniques is available. During the first six visits, I performed nerve glides of the dorsal, perineal, and inferior rectal branches of the pudendal nerve externally with Alexandria in a static position. Starting at Alexandria’s seventh visit, I had progressed her by performing the same nerve glides, but with passive movement of her left leg by bringing her left knee towards her chest (up to ~90 degrees of hip flexion range), which mobilizes her nerve more aggressively. We also continued to practice pelvic floor motor control and relaxation techniques. Her home exercise program consisted of very gentle nerve glides including anterior/posterior pelvic tilts as well as cat cow. By the eighth visit, she reported that her pain improved from eight out of ten to four out of ten. However, she stated that pain was still the worst with sitting/driving at six out of ten.
Since Alexandria denied pain with nerve glides accompanied with passive movements, I progressed by instructing her to perform the same movements but actively instead. Starting at her ninth visit, I manually distracted the connective tissue along her sitz bones to take pressure off the nerve as she performed active hip flexion and bridges to mobilize the nerve. For multiple sessions, she reported a reproduction of her symptoms at ~105 degrees of active hip flexion, but denied pain with active bridges. With each successive session, we worked towards achieving active nerve glides up to Alexandria’s end range, which we were able to with minimal pain at one out of ten by her 13th visit. At this point, Alexandria reported that she was able to drive for one hour, bend forward, and ride her recumbent bike twice (once for eight minutes and another time for 12 minutes) without pain. However, she stated that sitting for seven hours in front of her computer caused a “twinge,” but denied any significant pain.
Starting at her 14th visit, she reported onset of new symptoms, specifically sharp pain in her right hip aggravated by walking and ascending/descending stairs as there is also clicking in the hip joint. She stated that because her right hip was in so much pain, she started to bias her left leg more, which flared up her nerve-pain. She expressed that she was disappointed since she was doing so well up until this point. I reassured and educated her about how progress is never a linear path as there will be ups and downs throughout our journey towards recovery. For the next several sessions, I performed traction of the right hip to increase space and decrease pressure in the joint, which offered her significant relief. I also suggested she should reach out to an orthopedic doctor to get her hip checked out, then we discussed aquatic therapy as a therapeutic option for both her joint pain and nerve pain. With approximately three additional sessions, we were able to bring her pain back down to one out of ten from the current flare-ups she was experiencing. In addition, I was able to progress her home exercise program to perform nerve glides in a standing position and instructed her to work on a pain-free range of motion by considering both her nerve pain and hip pain.
At Alexandria’s 17th visit, she was able to tolerate static cupping along with movement of the cups on her left sitz bone without an increase in her symptoms. We also initiated nerve glides in a quadruped position with an active cat cow, which were tolerated well, so I was able to transition her treatment plan from weekly to once every 2 weeks due to her positive progress. At her 18th visit, she reported signing up for a gym and tried walking on the treadmill with a “tiny incline” to increase her activity levels, but unfortunately noticed that her nerve pain was aggravated two days later. She expressed confusion as she lives in an area with a lot of elevation and has not noticed her symptoms increase when walking up/down the hills around her house. I educated her about how the biomechanics of walking on ground versus on a treadmill are significantly different. By her 20th visit, Alexandria initiated aquatic therapy, so I collaborated with her aquatic physical and occupational therapists to ensure that none of the prescribed exercises conflicted with my treatment plan. Furthermore, I sent her home with some aquatic exercises to floss/glide the nerve with increased ranges of motion since this is usually tolerated better in the water than on ground.
For her next four visits, her pain levels were consistently one to two out of ten and only aggravated by forward bending when picking up cat litter off the ground. Therefore, I realized we needed to be more aggressive during our treatment sessions to get rid of the remaining pain. We started to perform passive and active standing nerve glides with static cups placed on her left sitz bone. For a passive glide, I instructed her to stand and bend forward at the trunk with her hands resting on the treatment table while I slowly lowered the table, which was tolerated well. As we progressed, I instructed her to stand and squat down within a pain-free range, then shift her weight side to side to glide the nerve with the cups in place. We also started to do internal treatment with increased left hip range of motion to allow me to address any trigger points deeper in the pelvic floor. She reported very minimal pain at one out of ten with these progressions, but we eventually had to stop the standing nerve glides during our session due to increased R hip pain from the squatting motions.
From visits 22 to 25, I transitioned her treatment plan from once every two weeks to once a month. However, at her 24th visit, Alexandria reported that she met up with her orthopedic doctor and an MRI of her hip confirmed a “labral tear in the right hip along with tendinitis of the hamstring tendon.” She planned for an upcoming corticosteroid injection and her doctor discussed the option of surgery if the injection is unsuccessful in reducing her pain levels. Fortunately, she reported that her right hip reduced from 10+/10 pain to zero out of ten after the injection. Despite her symptoms of right hip pain, she reported that her pudendal nerve pain has remained calm at one of out ten with sitting, driving, bending forward, and biking. Therefore, I discharged her at her 25th visit as she was given all the proper resources to self-manage her condition at home.
With the correct treatments and interventions, Alexandria’s pain and symptoms resolved within approximately nine months, which is a typical recovery time for nerve-related pain. She was provided with a thorough home exercise program to manage her condition, which consisted of diaphragmatic breathing, pelvic floor drops, foam rolling, stretches, and various nerve glides. I hope that those of you who are reading this are able to see that alleviating and managing persistent pain is very possible given the right guidance, resources, and mentality. If you would like to read more about how pelvic floor physical and occupational therapy can help with patients with pudendal neuralgia, you can do so via this blog.
Resources
Pudendal Neuralgia Resources [UPDATED]
______________________________________________________________________________________________________________________________________
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
In addition to virtual consultation with our physical and occupational therapistss, we also offer integrative health services with Jandra Mueller, DPT, MS. Jandra is a pelvic floor physical and occupational therapists who also has her Master’s degree in Integrative Health and Nutrition. She offers services such as hormone testing via the DUTCH test, comprehensive stool testing for gastrointestinal health concerns, and integrative health coaching and meal planning. For more information about her services and to schedule, please visit our Integrative Health website page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
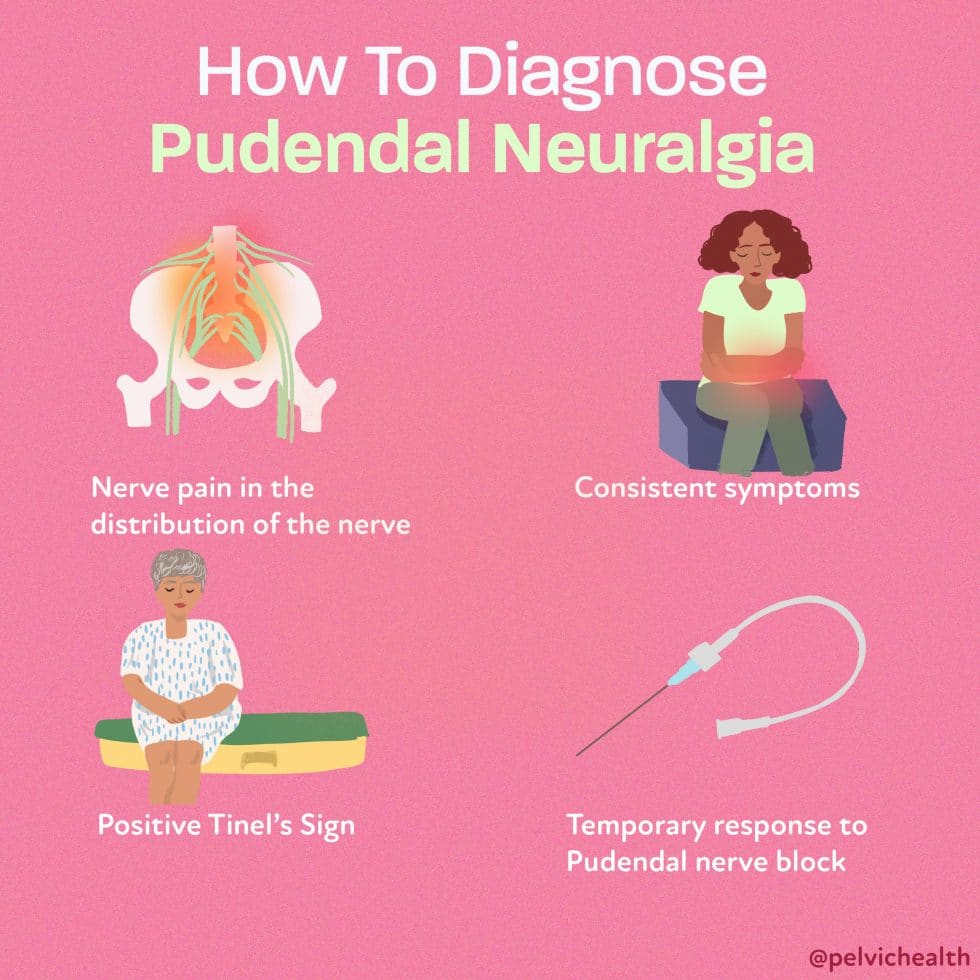
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.