
How Pelvic Floor Physical and Occupational Therapy Can Serve the Transgender Population: Part 1

By: Shannon Pacella
Earlier this summer, Dr. Heidi Wittenberg wrote a blog post enabling medical providers to understand transgender healthcare needs, which you can read here.
Following Dr. Wittenberg’s lead, I was fortunate enough to attend an educational course focused on the physical and occupational therapy evaluation and treatment of transgender patients, and I believe it is imperative to convey how important pelvic floor physical and occupational therapy may be for this population.
As Dr. Wittenberg had mentioned, some transgender individuals may decide to undergo gender affirmation surgeries in order to have their physical body align with their gender identity. These surgeries may include:
Female to Male surgical options:
- Chest reconstruction
- Hysterectomy with or without oophorectomy
- Metoidioplasty
- Phalloplasty
Male to Female surgical options:
- Breast augmentation
- Vaginoplasty
No matter which surgical options are or are not chosen, physical and occupational therapy plays an integral part of each patient’s care both pre and post operatively. I will cover how physical and occupational therapy can benefit patients preoperatively for those who do not wish to undergo gender affirmation surgery. Part two of this blog series will cover the role of physical and occupational therapy in the treatment after gender affirmation surgery.
Binding
Transmen might bind the breast tissue down (called binding) in order to create a flatter appearance prior to chest reconstructive surgery or binding may be done indefinitely without surgery. Binding incorrectly or not binding safely can result in long term impairments. It is important to remove the binder prior to sleeping and to only bind between eight to twelve hours per day.1 According to the article, “Health impact of chest binding among transgender adults: a community-engaged, cross-sectional study,” there were 28 health outcomes found as a result of chest binding, which included back pain, chest pain, bad posture, shoulder pain, numbness, and scarring.1 All of these impairments can be addressed through physical and occupational therapy. Proper education on posture is crucial for those who utilize chest binding. For those who wish to have chest reconstructive surgery, ensuring adequate muscle length in pectorals (which tend to be shortened with improper rounded shoulder posture) and good myofascial tissue extensibility around the chest is important prior to surgery in order to prevent complication postoperatively.
Packing
To create the appearance of a bulge in the genital region, transmen may perform packing with the use of a prosthetic. Packing may be used prior to metoidioplasty or phalloplasty, or it may be done without the end goal of surgery. There are various packing prosthetics available including: soft packers (used for aesthetic purposes), hard packers (can be used for penetrative intercourse), and stand to pee (STP) devices/packers (used to be able to urinate while standing).2 The packer is typically placed inside the underwear, some have specific underwear in order to adequately keep the packer in place. The use of any of these packers can affect how someone walks and can lead to adductor muscle tension if the person is constantly clenching their legs together in order to keep the packer in place. These impairments can be addressed with proper education from a physical and occupational therapists. In addition, if the stand to pee prosthetic is used, some may find it difficult to fully void while standing without straining. Over time, this may lead to urinary dysfunction including urinary hesitancy, incomplete voiding, and urinary frequency, and ultimately pelvic floor muscle dysfunction. It may be beneficial to consult a pelvic floor physical and occupational therapists if you are having difficulty using a stand to pee device.
Prior to Metoidioplasty
A metoidioplasty is a surgical procedure that lengthens a transman’s enlarged clitoris (testosterone induced) to create a penis/neophallus. The patient may elect to have urethral lengthening done as well, in order to be able to urinate while standing. The use of a clitoral pump may be indicated in order to maximize the size of the clitoris prior to surgery. Seeing a pelvic floor physical and occupational therapists to ensure unrestricted connective tissue and myofascial tissue around the suprapubic region and bony pelvis, and good pelvic floor motor control is important prior to metoidioplasty.
Prior to Phalloplasty
Transmen may decide to have a phalloplasty done, which is a surgical procedure to create a penis/neophallus, urethral lengthening, and optional scrotoplasty with testicular implants. There are many different surgical techniques to perform a phalloplasty, but most require taking a flap with nerve and blood supply as well as a skin graft to cover where the flap was taken from another area on the patient’s body, in order to have enough tissue to create the neophallus. The most common areas to take a flap for a phalloplasty are the radial forearm and latissimus dorsi region. The most common areas for a skin graft to be taken are the gluteal fold, abdomen, and thigh. Both areas (where the flap was taken and where the skin graft was taken) can end up with severe scarring and scar tissue formation that if left untreated could lead to pain, postural changes, and underlying muscle dysfunction. Prior to the phalloplasty, it can be very beneficial to the patient to seek out a pelvic floor physical and occupational therapists trained in manual connective tissue and myofascial release to work on the areas of the body that will be used for the flap and skin grafts to allow for adequate tissue length. Good pelvic floor muscle tone and motor control should also be obtained prior to surgery.
Tucking
Transwomen may perform tucking, which is a technique used to hide external genitalia and provide a smooth appearance. This involves tucking the testicles and penis between the buttocks; the testicles may be pushed into the inguinal canals as well. Some people use tight fitting underwear, an undergarment called a gaffe, or adhesive tape to hold the genitals in place, but this comes with some risks.3 Due to the placement of the urethral orifice close to the anus when tucking, there can be an increased risk for developing urinary tract infections as well as compression of the urethra leading to urinary dysfunction.3 Tucking for extended periods of time may lead to symptoms of prostatitis, epididymitis/epididymo-orchitis, and cystitis, which can lead to pelvic pain and pelvic floor muscle dysfunction.3 If someone develops pelvic pain or urinary dysfunction from tucking, they should consult with a pelvic floor physical and occupational therapists to assess these impairments and treat any connective tissue/myofascial restrictions and possible postural changes at the pelvis, typically excessive anterior pelvic tilting used while tucking.
Prior to Vaginoplasty
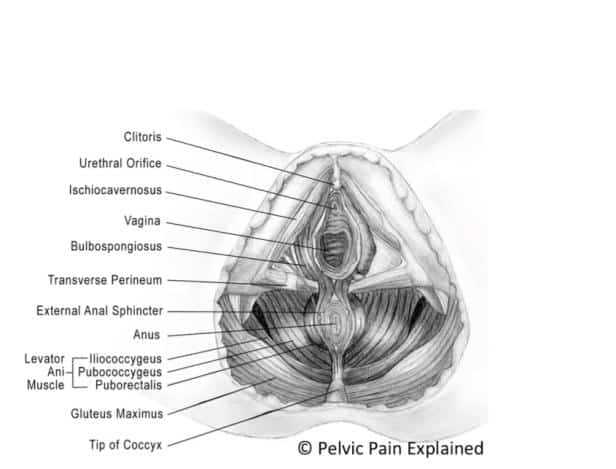
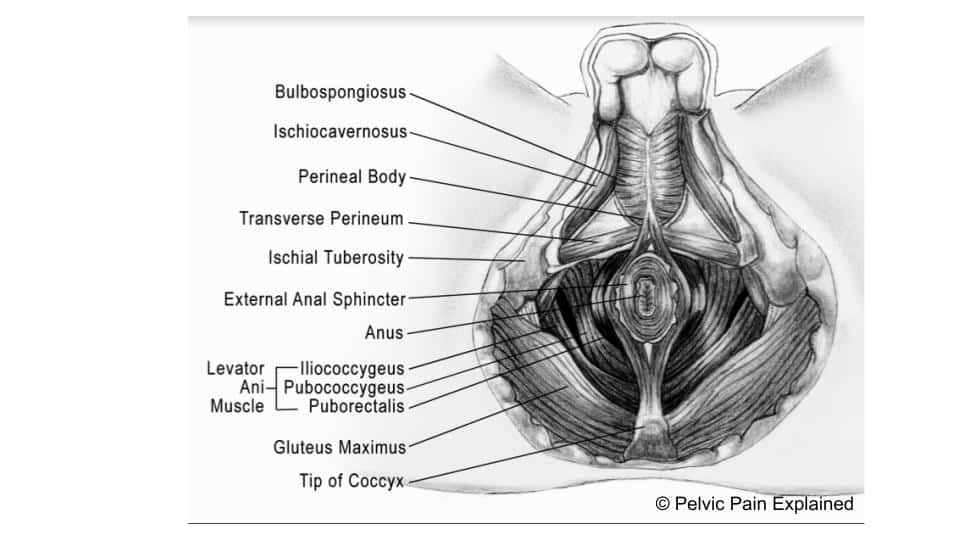
A vaginoplasty is a surgical procedure done for transwomen in order to remove the external genitalia (penis, scrotum, and testicles) and the creation of a neovagina. Due to the complexity of this surgery, the better a patient’s pelvic health is prior to the procedure, the better outcomes they may have. It is important to note that the bulbospongiosus muscle is removed during all types of vaginoplasties, and the levator ani muscle are partially dissected to improve vaginal canal width. You can visualize these muscles in the pictures above. If there is underlying pelvic floor muscle dysfunction or hypertonicity, it may be exacerbated post surgery; this is something that can be addressed by a pelvic floor physical and occupational therapists in order to improve the recovery process.The urethra is shortened significantly during this surgery to about one fifth its natal length, which may lead to urinary hesitancy, difficulty voiding, urinary urgency/frequency, and pain with urination. Pelvic floor motor control exercises are very important to practice, especially bulging and dropping in a sitting position, since the patient will need to sit while urinating after the vaginoplasty. Practicing urinating while sitting before the surgery can allow the patient to gain better control and feel confident post surgery.
As you can see, there are many aspects in which pelvic floor physical and occupational therapy can help the transgender population prior to gender affirmation surgeries, as well as for those who do not wish to undergo any surgery. At PHRC, we believe that good pelvic health is important for overall well-being as it affects many vital functions including urinary/bowel/sexual function, posture, and movement. Everyone should have the opportunity to work on optimizing their pelvic health no matter what, and we at PHRC are here to help!
Resources:
- Peitzmeier S, Gardner I, Weinand J, Corbet A, Acevedo K. Health impact of chest binding among transgender adults: a community-engaged, cross-sectional study. Cult Health Sex. 2017 Jan;19(1):64-75. Epub 2016 Jun 14.
- Underwood T. A Guide to Packers for Transmen. FTM Guide. May 9, 2016. http://ftm-guide.com/guide-to-packers-for-transmen/.
- Zevin, B. Testicular and Scrotal Pain and Related Complaints. Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/trans?page=guidelines-testicular-pain.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.


This is a very helpful post—thanks! Question: can taking hormones influence the pelvic floor muscles and exacerbate pre-existing pelvic floor dysfunction / hypertonicity / spasticity / pelvic pain?
Author Shannon Pacella says:
Hi Carmilla,
That’s a great question, there has not been very much research specifically looking at pelvic floor muscle changes with systemic hormone therapy in the transgender population. However there are some general pelvic and sexual health changes that have been studied that may influence underlying pelvic floor dysfunctions:
Systemic Estrogen:
Erectile function and capacity diminished – reduced or completely eliminated ejaculate.
Decreased libido/sexual desire.
Changes with orgasm response/sensation – whole body experience.
Systemic Androgen Blockers (ex: spironolactone) – may be used in conjunction with Estrogen :
Reduces orgasm ability/reduced libido.
Can cause increased urinary frequency.
May cause orthostasis/dizziness.
Systemic Testosterone:
Increased clitoral size and sensitivity.
Increase in sexual desire/libido.
Changes with orgasm response/sensation – more genital focused with higher peak intensity.
Urogenital atrophy, genital tissues may be more friable, more susceptible to fissuring.
Possibility of testosterone induced dyspareunia – may benefit from topical estrogen use at atrophic tissues.
Increased susceptibility for bacterial vaginosis.
Decreased lubrication – may contribute to discomfort with penetrative intercourse.
For further information, here are some helpful resources:
https://transcare.ucsf.edu/hormone-therapy
http://transhealth.ucsf.edu/trans?page=guidelines-pain-transmen
Best,
Shannon Pacella, PT, DPT
That’s interesting! And this article is quite helpful and do think I will be trying to do kegel excercises or something!
When I was a child, I took a few years longer than most to outgrow wetting the bed at night, and when, at age 31, i began feminizing HRT, at some point at around age 32 i began to have a bedwetting problem which has since come and gone and has been mostly getting better recently as I’ve started processing some things more.
When i reported the problem to some close internet friends, one suggested kegel exercises and i’ve been meaning to get around to them for months now. I think perhaps i was avoiding it due to dysphoria, but i’m ready to try them now. I believe they sent me some information on it.
Anyway I know it’s just anecdotal and could be related indeed as well to just general stress, but i thought my post-hrt bed wetting was worth sharing in relation to the other person’s question and your response.
Take care anyone who reads this!
Shannon can you please tell me what course you took and through what institution? I am looking to educate myself on this subject. Thank you in advance.
Hi Katherine,
Please see below link:
https://www.eventbrite.com/e/pt-evaluation-treatment-of-transgender-patients-tickets-42947451985#