How Pelvic Floor Physical and Occupational Therapy Helps Fecal Incontinence
Loss of bowels can be quite alarming considering a recent systematic review revealed that nearly 7.7% of community adults, with no difference in gender, have fecal incontinence.2 Fecal incontinence is defined as an uncontrolled loss of stool and can have significant implications on one’s physical and psychological well being. It is associated with social isolation, anxiety, loss of employment and declined self-esteem.1,2 The cause of fecal incontinence is oftentimes multifactorial. Some associated risk factors for fecal incontinence include:
- Weak or dyssynergic/uncoordinated pelvic floor muscles
- Pregnancy and childbirth
- Internal or external anal sphincter injury or dysfunction
- Radiation and/or surgery of the pelvis for cancer treatment
- Impaired rectal sensation
- Increasing age
- Urinary incontinence
- Poor bowel habits
- Fecal urgency
- Functional GI disorders such as IBS
- Watery stool or diarrhea
Because there are many contributors to fecal incontinence, it is important to consider the pelvic floor when problem-solving through treatment. The pelvic floor is a group of interconnected muscles that play a key role in providing stability and supporting our pelvic organs. If these muscles become weak or if their motor control is impaired, it may limit their ability to appropriately contain urine or feces. If this is the case, supervised strengthening and retraining of the pelvic floor and deeper core muscles with a physical and occupational therapists is warranted. A physical and occupational therapists may also perform rectal sensitivity for those patients that have difficulty recognizing fecal urge. In addition to retraining, your physical and occupational therapists will likely want to address your food, fluid and bowel habits. What you eat and drink and how you prep or position yourself for a number two can impact the consistency and frequency of your bowel movements.
Emptying your bowels up to three times a day to three times a week, given that the consistency of your stool is neither too hard or loose, is considered “normal.” Of course there can be deviations from this, but I would suggest checking out Rachel’s hilariously informative blog on all things poop. In short, the stool should have the consistency of soft banana (see Type 3 – 4 below on the chart), be brown and rest at the bottom of the toilet bowl. Foods “containing incompletely digested sugars, sweeteners, carbonated beverages, caffeine, alcohol, cured or smoked meat, spicy, fatty and greasy foods” can be irritable and create loose stools that may be difficult to control. Keeping track of what you put into your body and when you experience fecal incontinence may help you determine if any of these foods or others may be irritable to you. If you are still uncertain, consulting with a dietitian or nutritionist can be helpful. Additionally, adding in a bulking fiber or fiber with a high-water holding capacity like psyllium husk or chia seeds can help firm up loose stool. If you you decide to introduce a bulking fiber into your routine, remember to start small and then build up as necessary. You’ll also want to make sure you drink a glass of water with your daily fiber and get adequate water intake – half your bodyweight in ounces.
In addition to firming up your stool, getting in the habit of practicing healthy bowel habits may help with preventing fecal accidents. This may include preparing for and positioning during a bowel movement. I frequently have my patients practice an abdominal massage, following the path of the large intestines daily around the same time everyday to help stimulate the bowels. I also recommend that when having a bowel movement they are in a supported squatting position, with the hips lower than the knees. This position helps place the rectum in a more vertical position, providing a more direct path for the feces. The idea of improving the consistency of your stool and getting in an ideal position to empty your bowels is important – if you can empty your bowels sufficiently there will be nothing left to leak!
Assessing pelvic floor muscle strength and coordination, diet and bowel habits are a good first conservative step to treating fecal incontinence. While still experiencing fecal incontinence, wearing protective padding and utilizing a barrier cream will be important for maintaining pelvic hygiene. One may also consider utilizing an anal plug or a vaginal bowel control system (device inserted vaginally that “closes off” the rectum) for short-term use.2 If symptoms persist past conservative management there are pharmacological, surgical and neuromodulatory treatment options that also exist.
References:
- Meyer I, Richter HE. Evidence-based update on treatments for fecal incontinence in women. Obstet Gynecol Clin North Am. 2016;43(1):93-119.
- Ng KS, Sivakumaran Y, Nassar N, Gladman MA. Fecal incontinence: community prevalence and associated factors — a systematic review. Dis Colon Rectum. 2015;58(12):1194-209.
FAQ
What are pelvic floor muscles?
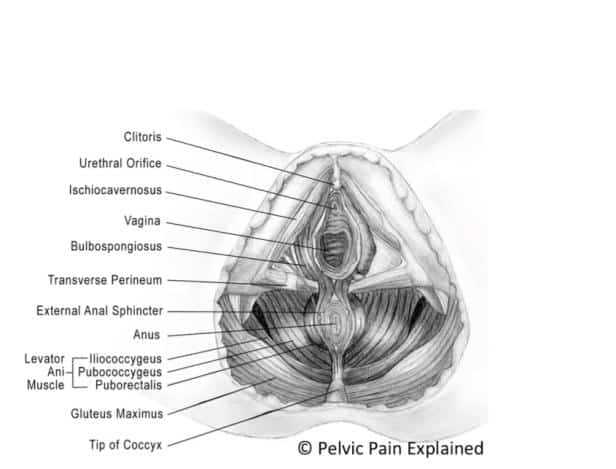
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Leave a Reply