
By: Elizabeth Akincilar, PHRC Cofounder
Explaining to someone who has never heard of pelvic floor physical and occupational therapy what type of physical and occupational therapy I practice is always an interesting conversation. People usually assume certain things about my practice. Most assume I primarily treat older women with “bladder issues” and new moms. People are always surprised to find out that almost 50% of the population I treat are men! Newsflash folks! Men also have a pelvic floor! Therefore, they can, and do, also suffer with pelvic floor disorders.
There are many reasons why men develop pelvic pain, but I’m going to focus on one particular cause for this post. Hernias. In particular, inguinal hernias. What are they? Why do they happen? How can they cause pelvic pain? How are they treated? How can physical and occupational therapy help?
An inguinal hernia is when tissue protrudes through a weak spot in the abdominal muscles. This bulge can be painful, particularly with coughing, bending over, or lifting something heavy. Typical symptoms are pain and/or pressure in the groin (inguinal canal), pain around the pubic bone, base of the penis, and/or testicles and occasionally pain upon ejaculation. A hernia is usually not dangerous, but can be if it becomes strangulated; therefore, it should always be evaluated by a physician. A few years ago Dr. Towfigh, a hernia specialist in Los Angeles, wrote an excellent blog post for PHRC on how she diagnoses a hernia. Check out her post for a quick review.
Hernias can occur without a cause. However, most are caused by an increase in abdominal pressure such as during straining with urination or bowel movements, chronic coughing or sneezing, pregnancy, and strenuous activity. Some people have a pre-existing weakness in their abdominal wall which makes them more susceptible to developing a hernia.
We mostly see men with hernias because men are eight times more likely to develop an inguinal hernia than women are. Sorry guys! Other risk factors include being caucasian, chronic coughing, chronic constipation, a family history of inguinal hernias, and just being older because muscles weaken as we age. So, if you’re an older white dude that is chronically constipated and smokes, an inguinal hernia is likely in your future.
If the hernia is small and not causing discomfort, treatment may not be necessary. Watchful waiting may be sufficient. However, if it is causing significant discomfort, a surgical repair is typically indicated.
I’m sure you’re wondering where physical and occupational therapy fits into this scenario since I just told you surgery is the most appropriate treatment for inguinal hernias. It turns out that approximately 25% of people that undergo hernia repairs experience chronic (lasting longer than three months) groin pain after surgery, with 10% of those people reporting moderate or severe pain.1 It is this group of patients, typically men, that look to physical and occupational therapistss for conservative treatment to help them decrease their pain.
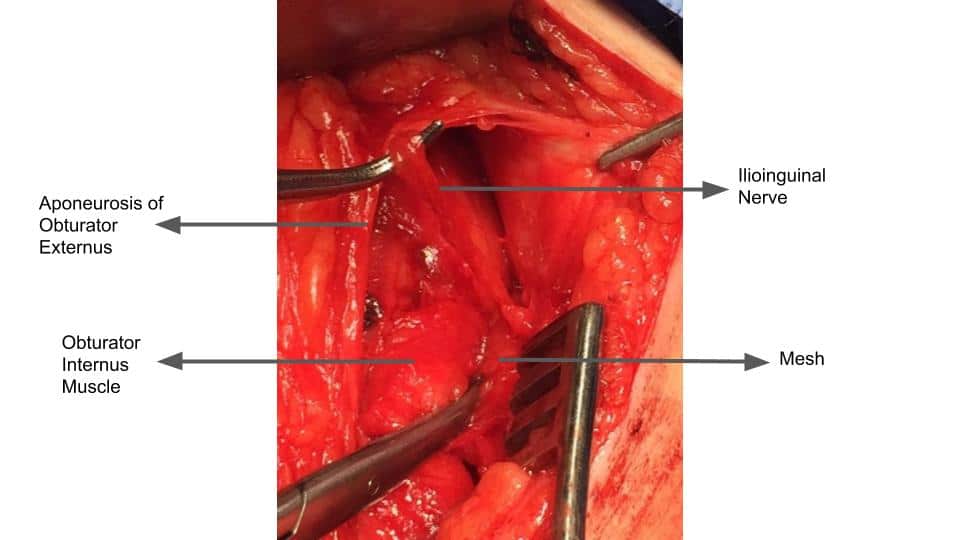
Persistent pain after a hernia repair can have several causes. There are two primary surgical techniques to repair inguinal hernias: laparoscopic and open. Both surgical methods can potentially injure nerves, specifically, the ilioinguinal, genitofemoral, and iliohypogastric nerves. All three of these nerves travel close together, in part, along the inguinal canal. To make things more complicated, anatomic variation is fairly common with these nerves. Meaning, in some people, the nerves aren’t exactly where they are expected to be. Therefore, during surgery, one, or more, of these nerves may be more susceptible to injury. Additionally, the vast majority of hernia repairs utilize mesh to close the hernia. The mesh itself can be a source of persistent pain. The surgical tacks used to affix the mesh to the pubic tubercle can also cause pain. Lastly, the surgical scars themselves can cause pain.
Physical therapists utilize soft tissue mobilization techniques to decrease persistent pain after many surgical procedures, including hernia repairs. With manual therapy, we can improve the mobility of the surgical scar and the surrounding muscle and fascia. Mobilizing the scar will decrease pain coming from the scar itself. As scar tissue forms around the mesh, the mesh becomes very stuck to the surrounding fascia and muscle. As a person bends, lifts, or coughs, the stuck mesh can cause pain because it’s yanking on surrounding muscles, tissue and nerves. Ouch! Improving the mobility of the muscle and fascia around the mesh can decrease that pain. Lastly, improving the mobility of these soft tissues will create more space for, and decrease tension on, the surrounding nerves that may have been negatively affected during surgery. With manual therapy, we can help to normalize the mobility of these nerves so they can slide, glide, and stretch normally. Manual therapy also decreases ischemia (improves blood flow) for these nerves facilitating healing, and ultimately decreasing pain.
In addition to physical and occupational therapy, the patient may also benefit from interventional pain management, such as a nerve block, to the affected nerve or nerves. In the case that conservative therapy does not reduce the pain sufficiently, a neurectomy, may be indicated. A neurectomy is a surgical procedure that cuts the involved nerve to reduce pain. Dr. Linn, a surgeon from Chicago, reviewed these interventional pain management options as well as surgical treatment options for patients suffering from persistent pain after hernia repair, at the 2018 International Pelvic Pain Society Meeting. Read a summary of his lecture here.
As I mentioned at the beginning of this post, inguinal hernias are only one cause of pelvic pain in men. In May, which is Pelvic Pain Awareness Month, PHRC will present our first Pelvic Pain Pow Wow! This will consist of five video webinars, one every week in May, each focusing on a different aspect of pelvic pain. Follow us on Instagram for more information about our Webinar series. Tune in the week of May 20th as I review other causes of male pelvic pain and how pelvic floor physical and occupational therapy can help.
References:
- Poobalan AS, Bruce J, Smith WC, et al. A review of chronic pain after inguinal herniorrhaphy. Clin J Pain 2003;19:48–54
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
Unbelievable. This sounds like exactly what has been bothering me for 7 years, since I had my prostate removed. I’m going to get this checked out. Thanks.
What a lovely blog page. I will definitely be back again. Please keep writing!