Photo via Joe Loong via Flickr
In previous entries, Britt beautifully took us through all things posture (Posture and the Pelvis Part One and Part Deux). Here are some important takeaways from her posts to consider as we explore how sitting may affect your pelvic floor:
- The diaphragm, trunk (back extensors, transversus abdominis, obliques, etc.) and pelvic floor muscles are all part of your ‘core’
- Posture is not a position you hold but rather a state of balance
- Base of support, alignment and pressure are essential to maintaining your state of balance
- Sitting, standing or moving outside your state of balance can change the ideal length-tension ratio
- Altering the length-tension ratio can shorten or lengthen the muscle making them appear weak and less efficient
- Posture is dynamic and dysfunctional holding or movement patterns can manifest as or exacerbate pelvic symptoms
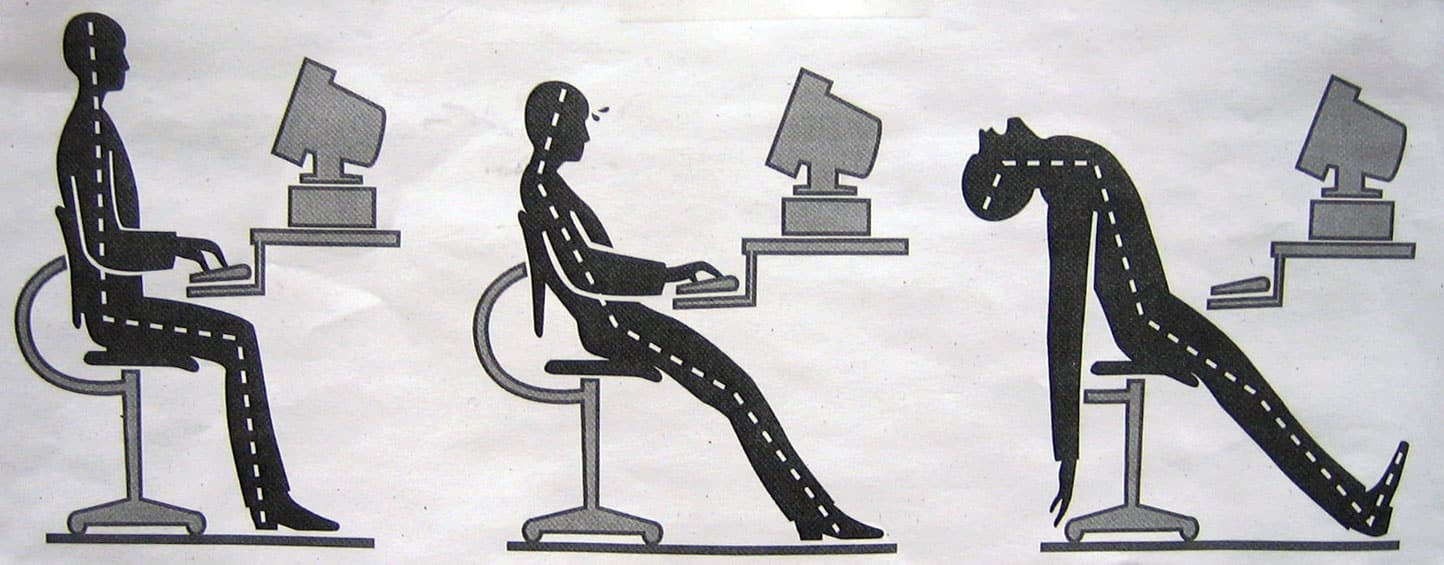
As you can see, posture is not as simple as “standing tall” or “sitting up straight.” Positioning your body in poor posture, especially for prolonged periods of time can lead to a breadth of pelvic floor dysfunctions. This may include pain with sitting, coccydynia, low back pain, urinary frequency, incontinence, etc. Living in the Bay Area, a world of technology, finance and commutes I come across many patients with the hallmark slumped sitting posture – their heads, shoulders and low back are all rounded forward. It is not uncommon for me to hear at a patient’s first visit, “I sit eight plus hours a day at work” or “I travel two hours one way to get to the office” or “I frequently fly across the country for my clients.” Whichever the response, this is too much sitting and could potentially lead to dysfunction later down the road.
It has been cited in numerous studies that sustained pressure can lead to mechanical deformation and tissue ischemia with muscle being the most susceptible tissue.2 These reactions also occur in the skin and other subcutaneous tissues especially around bony prominences. In regards to sitting this may include your sitz bones, tailbone, sacrum or low back. Here are two illustrations of how this may impact pelvic symptoms:
Mechanical deformation → altered muscle length-tension ratio → inefficient functioning muscles → frequency, incontinence, pain, etc.
Ischemia → less blood flow → decreased oxygen → pain
So how often should one take a break from sitting? In a systematic review addressing pressure ulcers in patients with spinal cord injuries, authors reported that it takes approximately two minutes of pressure relief to unload transcutaneous tissue and raise local oxygen perfusion. They suggest this be performed every fifteen to thirty minutes.4 Unfortunately, this is unrealistic for the working person and thankfully we tend to shift as we sit anyways. As a rule of thumb, I typically recommend patients get up at least every hour or so and walk at least two minutes.
The Centers for Disease Control and Prevention (CDC) also recognize the consequences of prolonged sitting and have even piloted studies for intervention in the workplace. Though they do not site specific pelvic symptoms due to prolonged sitting, the CDC has reported correlation with premature mortality, obesity and many chronic conditions such as cardiovascular disease and diabetes. No worries though, it appears that taking frequent breaks from sitting may lower these health risks. In the CDC’s Take-a-Stand Project, individuals that had access to a standing workstation reduced their sitting time by 224%; 66 minutes a day. They also reported reduction in upper back and neck pain and even improvements in their mood.3 It’s important to also note that those who were provided a standing desk did not stand all day. The key is to find a balance of standing, sitting and moving.
If your company offers an ergonomic assessment, DO IT! If not, push for it. If still unsuccessful, you can follow these tips for general sitting posture:
- Maintain the natural s-shaped curve of your spine with your head slightly tucked and shoulder rolled down and back
- If able, hands should be positioned up vs. down to facilitate external rotation of your shoulders to prevent rounding of your shoulders and head
- Lumbopelvic position in neutral with weight centered equally on both sitz bones (*more on this below)
- Ideally, your hips should be slightly higher than or in line with your knees, creating a 90 degree angle
- The back of your thighs should be in contact throughout the seat of the chair vs. the edge of chair. This distributes the pressure over a larger surface area, decreasing the demands of any one area of your thighs or buttocks
- Feel flush with floor or a stool if on the shorter side and equal weight bearing through your feet
Kaiser Permanente has a pretty awesome interactive page with detailed explanation on how to incorporate these tips in the workplace i.e. ergonomics. I highly recommend you check it out.
*A little more on neutral pelvis…
Maintaining a neutral pelvis in sitting can have a great impact on keeping your pelvic floor healthy and efficient. Why is this so important and how can you achieve a neutral pelvis? As we mentioned before, your pelvic floor muscles are one of your postural muscles, they are essential to maintaining your balance. They create this bowl that slings from the pubic bone and attaches back onto the tailbone and sacrum. In addition to keeping you stable, the pelvic floor muscles also play an important role in supporting the internal organs (bowel, bladder, prostate and uterus). When you fall outside a neutral pelvis, you alter the length-tension ratio of the pelvic floor muscles. This may either shorten or lengthen the pelvic floor muscles, making them less efficient. Tight or overstretched muscles can either create pain or make it difficult to support the internal organs. Let’s use the urinary system as an example. If your pelvic floor muscles are hypertonic, this may give you feedback that you have to urinate even though you may have nothing to void. There is only so much space within the pelvis so when the pelvic floor muscles are resting in an “up and in state” it can make you feel like you have to pee. On the other hand, if you pelvic floor muscles are positioned in a lengthen state, they can exacerbate feelings of vaginal heaviness or incontinence as they are not properly supporting the bladder or urethra.
Having a neutral pelvis also means maintaining the natural concave curve of the lumbar spine. Oftentimes in clinic, most patients are flattened or rounded in their low back (hypolordotic) but we have also seen patients that are excessively arched (hyperlordotic). What does this mean for the pelvic floor? In a study out of Canada, researchers looked at the impact of lumbopelvic position on the pelvic floor muscles in standing. All participants (healthy, nulliparous women ages 22 – 41) performed five different tasks (static standing, maximal effort cough, Valsalva maneuver, maximal effort voluntary pelvic floor contraction and a load-catching contraction) in three different lumbopelvic positions; normal lumbopelvic posture, hyperlordosis and hypolordosis. Electromyographic (EMG) activity was collected using a vaginal sensor to monitor the activity of the pelvic floor and external sensors were placed on the trunk muscles (rectus, external and internal obliques and erector spinae). Interestingly, EMG activity in standing hypolordotic was higher than normal posture. During activities of maximum pelvic floor contraction, cough, Valsalva and load-catching there was less EMG activity for the hyperlordotic and hypolordotic positions compared to normal.1 What might this information suggest? (1) Strengthening of the pelvic floor muscles may be more effective in a neutral position for patients that have low tone and (2) patients that are chronically holding oftentimes in a hyperlordotic posture, may be perpetuating their dysfunction by placing excessive pressure on internal organs.
So, how do you find neutral? To find your neutral pelvis in sitting, try shifting your pelvis forward (anterior tilt) and backwards (posterior tilt). The goal is to find the balance between these two positions. As you are shifting your weight, you are looking for the position in which you feel pressure equally beneath your sitz bones. You will also feel slight tension anteriorly at your pubic bone. This is neutral. The position where your pelvic floor muscles are most efficient. If you are cleared to kegel, one way you can test this is by kegeling in each position. Notice that when you perform a kegel in either an anterior or posterior tilt, the range of motion of the pelvic floor muscles is less. That is, the pelvic floor muscles travel a shorter distance up when contracted and down when relaxed. When you are truly in neutral, you will feel as though you have a stronger contraction likely because the pelvic floor muscles are now able to move through their entire available range of motion.
While first practicing these new positions, you WILL feel off. That’s expected. You are teaching yourself a new way to be in your body. The brain is a marvelous organ but can cling on to what it already knows. You will likely have to “check in” but eventually you will find a new normal that will help you engage the appropriate muscles to keep you balanced. If you are having difficulty using these tips for optimal seating posture and are also experiences pelvic floor symptoms, we would love to see you! With years of holding, there may be myofascial restrictions (i.e. tight hamstrings, pecs, etc.) that may make it difficult to successfully maintain the natural curves of your spine and a neutral pelvis.
References:
- Capson AC et al. The role of lumbopelvic posture in pelvic floor muscle activation in continent women. J Electomyogr Kinesiol. 2011;21(1):166-77.
- Cardenas, D & Dalal, K. Spinal Cord Injury Rehabilitation. Physical Medicine and Rehabilitation Clinics of North America. Pg. 643
- Nicolass Pronk et al. Reducing occupational sitting time and improving worker health: the take-a-stand project, 2011. Prev Chronic Dis 2012;9
- Regan et. al. A systematic review of therapeutic interventions for pressure ulcers after spinal cord injury. Arch Phys Med Rehabil. 2009;90(2):213-31
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
Are there any exercises that can be done to help fix this kyphosis if you must work at an office desk for multiple hours each day? I feel that maintaining great posture is obviously important for the reasons in your article, but it is hard to do so for so long.
Author Nicole Davis says:
Hi John! Typically with kyphosis and a rounded upper trunk you need to lengthen the muscles in the chest (pectoralis, scalenes) and strengthen the muscles in the back (rhomboids, latissimus dorsi, mid-lower traps). When trying to improve your posture from previous holding patterns, it’s oftentimes difficult to maintain if you have not done both the lengthening and strengthening of the appropriate muscles because 1) short muscles in the front will pull you back in and 2) weak muscles in the back will get tired. I would recommend doing an initial consultation with a physical therapist to get a better idea on which muscles need to be addressed in your case and if there are any skeletal contributions to the kyphosis.
What a great summary of a large and complex subject!. Thank you.
I am constantly thought about this, thanks for putting up.
Thanks for sharing your thoughts on holiday. Regards