
Pudendal Neuralgia Series 1: Interdisciplinary Conversations from IPPS 2015

By Stephanie Prendergast
Pudendal Neuralgia seems to be a diagnosis that is more polarized and controversial than other pelvic pain diagnoses.
Why?
Over a series of posts we will look at the evolution of this diagnosis, and why we need the perspective of a pelvic floor physical and occupational therapists, pain management specialist Dr. Sheldon Jordan, and gynecologist/pelvic pain specialist/pudendal surgeon Dr. Mark Conway, to explain how to manage this literal pain in the ass.
This week we hear from Stephanie:
When PN was first described in 1988, it was viewed as a compression entrapment syndrome, similar to carpal tunnel syndrome. The treatment protocol consisted of three corticosteroid nerve blocks, medications, relaxation therapy and then surgical decompression. Pelvic floor physical and occupational therapy was not an option or part of the treatment protocol.
A lot has changed since 1988.
Our colleagues in Nantes, France were one of the first groups to develop a surgical decompression procedure for the pudendal nerve. In a paper published in the European Journal of Urology, they reported that between the years of 1988 and 2004 they evaluated over 700 number of patients with PN and performed surgical decompression on 400. They decided to perform a prospective study comparing surgical decompression to conservative care, published in 2005. (1)
Conservative care consisted of pudendal nerve blocks, medication, and relaxation/biofeedback therapy. The surgical group was given the same treatment options as the conservative group and surgical decompression. Initially 16 people were in each group.
Surgery was considered a ‘success’ if the self-reported measures include a 3-point reduction in a 10-point Visual Analog Scale. 50% group that had surgery showed a positive change in the VAS scores. 50% of the group the had surgery did not report enough a change to be considered a ‘success’. The group that received conservative care did not report a significant enough change to be be considered a “success”
These results left a lot to be desired, prompting the group to take a closer look at how they were diagnosing PNE. During that period of time, electrophysiological testing was being done to try to confirm a PNE diagnosis. They concluded that these tests are neither sensitive nor specific to identify PN by PNE and therefore CANNOT be used to confirm this diagnosis. (2)
This was GREAT news because these tests are so painful, they make a root canal seem pleasurable.
In their next paper, the Nantes team suggested clinical criteria that can be suggestive of PNE (3):
- Pain in the territory of the nerve.
- Pain is predominantly experienced when sitting.
- Pain does not wake the patient at night.
- Pain with no objective sensory impairment.
- Pain relieved by diagnostic PNB

The conclusion was that entrapment is one cause of Pudendal Neuralgia but other causes also exist.
Over the next several years, the volume of papers describing the role of the pelvic floor and girdle muscles in pelvic pain syndromes increased exponentially. It turns out the majority of people with pelvic pain have neuromuscular abnormalities that are contributing to their pain. Along with other diagnoses such as Vulvodynia, Interstitial Cystitis, and Chronic Nonbacterial Prostatitis, Pudendal Neuralgia became classified as a neuromuscular and/or neuropathic pelvic pain syndrome, changing how it is diagnosed and treated.
Everyone with PN has asked the question, why did I get this when someone else doing the same thing did not?
We recognize now that certain people may be anatomically predisposed to developing a neuralgia. Impairments and pain develop when a particular event exceeds what that individual’s body is capable of handling. The particular event may seem as benign as sitting, but if your pudendal nerve is running through the sacrotuberous ligament, sitting on a chair may feel like you are actually sitting on a fire poker. Thus, a particular person’s activities, comorbidities, genetics, etc or a combo of all or some of the above can create a ‘perfect storm’ and wreak havoc.
Of note, 30% of the average population has an “entrapped” nerve in cadaveric studies. This means that 30% of the population could be vulnerable to developing a neuralgia when entering that “perfect storm”. However, clearly 30% of all people do not have neuralgia. The cadaveric studies show that abnormalities can exist without symptoms. Therefore, a differential diagnosis is necessary to determine the right course of treatment for the particular person in question. Additionally, the impairments associated with PN can be divided into two broader categories: a pain impairment (central nervous system) and peripheral dysfunction (nociception).
I should emphasize that pain and peripheral dysfunction are not the same and both need to be addressed for a successful outcome.
The Biopsychosocial Approach to PN
Sandy Hilton, MS PT and Caroline Van Dyken, BHSc,PT, Cred MDT CCMA (Acup) beautifully describe a comprehensive framework to managing pelvic pain syndromes such as pudendal neuralgia: “The framework integrates the current understanding of local tissue dysfunction with the wider context of sensitized protective mechanisms within the spinal cord and brain. Treatments address both the local tissue complaints and the central nervous system sensitivity by teaching patients about the biological processes underpinning their pain, graded imagery, and graded exposure”. (4)
We cannot ignore the mind while we treat the body. Sometimes the body isn’t ready to be treated until the mind is managed. Other times, physical and occupational therapy for the body and psychotherapy for the mind are not effective until the pain is better controlled by therapies directed at the central nervous system. Every now and then, we need surgery.
What I hope is clear, is that there is no standard protocol for treating PN.Every case of PN is different, even if two individuals have the exact same symptoms. The trick is to identify which impairments are the predominant problem in each person, and then develop an effective strategy to treat these impairments.
I repeat my statement from last week’s blog: It is the norm, not the exception, that people getting on the path to healing will fail to respond or not tolerate at least one medication, procedure, physical and occupational therapy session or series. It is not uncommon for symptoms to persist, and or reappear. The good news is that if this is happening to you now, you and your healthcare providers can troubleshoot and overcome treatment challenges in an interdisciplinary treatment model!
This wraps up part one in our series. In the next post, we are will talk about the following common scenarios, NOT RESPONDING, and NOT TOLERATING treatment. Yes, talking about our successes is important. But, talking about our challenges is even more important. If we don’t, we’ll never achieve success.
We know you have questions and comments. On Thursday, November 5, 2015 at 6:00pm PST, Drs. Conway and Jordan and Stephanie will be interviewed on the Pelvic Messenger Radioblog. There will be time for questions and answers during this 75 minutes segment.
You can find the link to the show here: http://www.blogtalkradio.com/pelvicmessenger
Finally, here a couple of video snippets from my IPPS lecture, “Interdisciplina
Pain, Anxiety and Depression IPPS 2015
All my best,
Stephanie Prendergast, MPT

Stephanie A. Prendergast, MPT is the co-founder of the Pelvic Health and Rehabilitation Center, which has locations in San Francisco, Berkeley, Los Gatos, Los Angeles, and Boston. She currently treats patients in the Los Angeles location. Stephanie began serving on the International Pelvic Pain Society’s Board of Directors in 2002, served as their Vice-President and Scientific Program Chair in 2012, and in 2013 was the first physical and occupational therapists to serve as President. As an acknowledged leader in the field, she was invited to become on of the founding Board members of the Society for Pudendal Neuralgia in 2005 and subsequently co-developed and teaches “De-mystifying Pudendal Neuralgia,” a continuing education course attended by doctors, physical and occupational therapistss, and other allied health professionals around the world. She served on the program committee for the World Congress on Abdominal and Pelvic Pain in 2013 and 2015 and is also Co-chair of the program committee for 2017. She is internationally recognized authority in the field of pelvic floor dysfunction, lectures regularly, and has numerous publications in medical textbooks, journals, and magazines. She co-authored the book Pelvic Pain Explained, to be released in January of 2016. You can find her on Twitter @pelvichealth, on Facebook at facebook/pelvicpainphysicaltherapy, and subscribe to PHRC’s weekly blog at pelvicpainrehab.com/blog.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
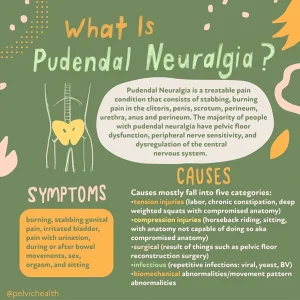
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Sitting pain started Nov. 2010. Tried my family doctor, gynecologist, 2 chiropractors, physical therapist that was recommended by my gynecologist and no one and nothing they tried helped. After 2 yrs. I had to find a new internal medicine doctor and on my first visit she sent me to a Phys. Therapist at Womens Advantage in Torrance, CA that treated the pelvic floor. I finally had someone explain my problem and she started treatment. She sent me to Long Beach, CA to a specialist in Women’s Pelvic Floor and I started receiving injections in the obturator and lipator ani muscles. What an improvement. A family illness caused me to postpone my treatments. I am just about to start again with Botox injections. Dr. Craig seems to think that this is the next step. I am apprehensive but so willing to try. With the break of treatment I have become so uncomfortable with the sitting again. My “sitter” muscles are so tight and hard again. Have had to give up a lot of physical things that were such a part of my daily life. I have not given up hope that things will one day be so much better. Bless you and all who work so hard to help the afflicted ones. Thank you, Edna
Hi Edna,
Stick with treatment, you can and will get better!
Hi Stephanie,
is the pudendal nerve considered a peripheral nerve? My Pudendal neuralgia has really calmed down after 4 years of various therapies, however I’m left with terrible allodynia. The front of my legs don’t tolerate clothing, my shins burn. Sandy Hilton mentions graded imagery above, would that be a helpful therapy for allodynia? My neurologists office knows nothing about it.
Any other ideas?
Appreciate your help,
Debbie
Hi Debbie,
The pudendal nerve is a peripheral nerve. Allodynia is not uncommon in people with PN. Sandy is correct in that graded imagery can help, as well as other desensitizing therapies. A physical therapist, psychologist, hypnotherapist or mindfulness expert may be able to help you based on their particular training.
Best,
Do you know of , or recommend specialists in the Toronto region?
Hi Noreen,
Please use the link below to find pelvic floor physical therapist.
https://pelvicguru.com/2016/02/13/find-a-pelvic-health-professional/
Regards,
Admin