
By Jandra Mueller, DPT, MS, PHRC Encinitas
SIBO, aka small intestinal bacterial overgrowth, is bacteria that is an overgrowth of the normal bacteria in your small intestine.
In today’s blog I want to provide some more education about SIBO, how we get it, test for it, treat it, and how it has made its way into pelvic health concerns as well as the most recent updates.
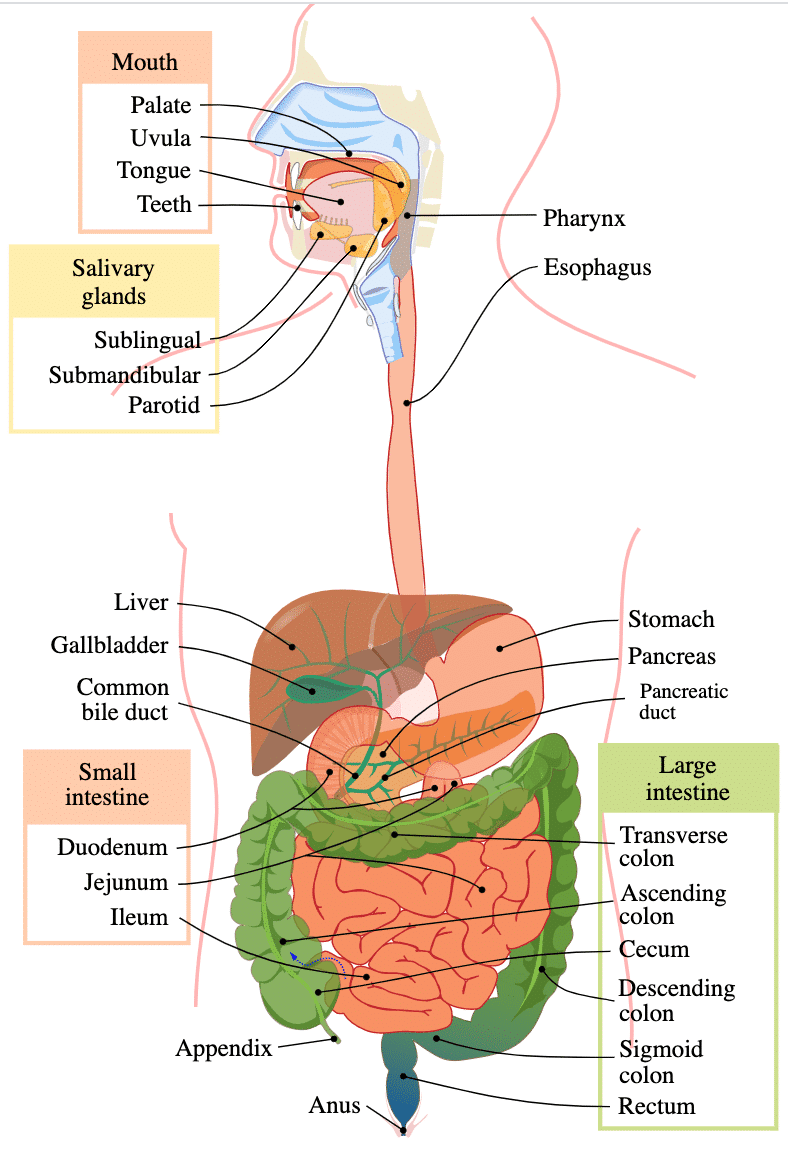
GI Anatomy
First, it is helpful to know a little bit about the digestive system aka your GI tract, and anatomy before diving into more SIBO facts. Your GI tract begins in your mouth with your tongue and all the enzymes that are in your saliva that help to break down food. Then, food travels down your esophagus into your stomach where it is further digested. Acid helps to kill bacteria and help with protein digestion as well as other processes to help with B12 activation and absorption. Then food moves into your small intestine, where you continue to digest your food and absorption of nutrients begins (hint: this is where SIBO occurs!). Once this process takes place, food moves into your large intestine also known as the colon through the ileocecal valve where it can be used to feed all of the good bacteria that is supposed to be there, and it eventually gets moved through to the rectum and out of your body on a daily basis (hopefully!).
SIBO is essentially a subclassification of IBS and it has been reported that approximately >50% of the patients with SIBO have IBS (Chedid, 2014). SIBO is essentially the GI symptoms in the presence of overgrowth of hydrogen-producing bacteria in the small intestine. However, in many years it was also thought to be an overgrowth of methane-producing bacteria; however, recently there have been updates to distinguish this from classic SIBO which I will address in the updates section.
The classic symptoms and/or the associated issues with SIBO include:
- Abdominal bloating one to two hours after eating
- Gas, belching, and a feeling of fullness
- Diarrhea and/or Constipation* (We will talk more about this in the updates section)
- Brain fog
- Fatigue
- Food sensitivities and reactions (if intestinal permeability occurs)
- Poor nutrient absorption (B12, iron)
These symptoms occur because the bacteria that are overgrown love certain types of carbohydrates, ones that can be fermented, these are termed FODMAPs, or fermentable oligosaccharides, disaccharides, monosaccharides, and polyols. Many of you may recognize the term “the low FODMAP diet” and that is a diet many people are recommended to go on to help with symptom reduction.
Foods high in FODMAPs include:
- Garlic
- Onion
- Vegetables that include fructans, galacto-oligosaccharides (GOS), fructose, mannitol and sorbitol which include broccoli, cauliflower, asparagus, brussels sprouts, cauliflower, chicory leaves, globe and Jerusalem artichokes, karela, leeks, mushrooms and snow peas
- Fruits high in fructose like apples, apricots, cherries, figs, mangoes, nectarines, peaches, pears, plums, and watermelon
- Legumes: Baked beans, black-eyed peas, broad beans, butter beans, chickpeas, kidney beans, lentils, soybeans and split peas
It is important to note that these bacteria also respond to foods that are low in FODMAPs, but consumed in high quantities such as wheat and other fruits and veggies consumed in high quantities in the Standard American Diet also known as SAD. To find out more about the low FODMAP diet and foods that are high/low in FODMAPs, check out Monash University here.
Later in the blog, I will discuss some recent updates from Dr. Pimentel, who is one of the primary researchers and practitioners. He recently published an update on the clinical guidelines this year. One of the updates, though, was on methane vs. hydrogen SIBO. Methane-positive breath tests were previously considered SIBO; however, it is no longer classified as SIBO because methane-producing organisms are not bacteria, they are archaea. Therefore, the name SIBO which implies bacterial overgrowth is no longer accurate, and methane-positive “SIBO” is now called “Intestinal Methanogen Overgrowth” or “IMO.”
Why do we get SIBO?
As Dr. Pimentel has stated in various interviews SIBO is the result of some other underlying problem. Listed below are some of the primary causes and/or predisposing triggers for SIBO, the issues below are not listed in any particular order.
- Food poisoning. One of the main causes of SIBO has been tied back to a food poisoning event. Some may know the exact moment when you had to dash to the bathroom after that somewhat odd seafood when traveling abroad and others may have no recall of having a food poisoning incident.
- Heliobacter Pylori (H. Pylori). H. Pylori is a type of bacteria that infects the stomach and can be asymptomatic in many. However, it can cause damage to the stomach and the small intestine. It also produces an enzyme that lowers stomach acid which I will cover below.
- Low stomach acid (hypochlorhydria) and altered digestive secretions are another leading cause. Naturally, our stomach should be very acidic which helps to kill unwanted bacteria that enters our mouths on a daily basis. As we get older (even in our mid-late 30’s) our stomach acid begins to decrease naturally; however, this can occur for many other reasons such as malnutrition and poor caloric intake, chronic stress, chronic illness, eating under stressful conditions, and using proton-pump inhibitors and antacids for long periods of time. Hypochlorhydria presents similarly to indigestion and heartburn (but for different reasons).
- Adhesions are often another cause of SIBO in that they may restrict the intestines and cause an obstruction which can alter motility. This can be from other GI issues such as Crohn’s disease, surgery, and even endometriosis has been thought to potentially be a trigger for SIBO.
- Altered motility. The migrating motor complex or MMC plays a critical role. Normally between meals, there is essentially a wave of contractions or peristalsis that occurs to flush out everything in our intestines and keep things moving toward the colon. In many people with GI issues, this is altered. With slow transit through the GI tract, this allows bacteria to both thrive and grow as well as not get flushed out. Fast motility as in the case with some people with diarrhea causes alterations in our digestion and absorption as well. The majority of issues however are with slow transit. Motility agents and drugs can help with this slow transit and it is recommended to space meals further apart (four to five hours) which contradicts what many of us have learned about eating “small but frequent” meals.
- Chronic stress. This is because stress can play a role in how our GI system works overall. When we sit and eat under stressful conditions, this can lead to poor production of stomach acid and poor secretion of all those digestive enzymes that help us break down and absorb our nutrients and keep our bacteria in check. Chronic stress also lowers our immune system which makes it more difficult for our body to naturally prevent infection and disease.
Testing for SIBO & IMO
Most of the research that is done when studying SIBO uses a biopsy or culture of the small intestine which can then capture the number of bacteria present. This method is also used in some clinics that diagnose and treat SIBO but is not the easiest or most feasible to do. Typically a breath test is used either in the clinic or a take-home test is given.
The test uses a solution, glucose or lactulose (but usually lactulose), that is consumed and then one would blow into tubes at 20-30 min intervals which are then analyzed for the amount of hydrogen and methane gas that is expelled. If there is a specific amount of either gas at certain time points, the test is positive for overgrowth and there are a number of treatment options available.
The gold standard is the biopsy; however, this is not very easily performed; therefore, the breath test was created. The take-home test is, of course, the most convenient but it does require some preparation and planning and there can be high user error so it is important to have someone direct you on how to take this test to minimize user error.
Additionally, stool tests like the GI effects and GI-MAP can give us some indication about bacterial overgrowth and can also test for H. pylori. Of course, the GI symptoms that describe SIBO can also be other issues with the gut such as poor diversity in the microbiome and food sensitivities for instance. These tests allow for a more comprehensive assessment of the gut, looking at digestion and absorption, infection and inflammation, and overall gut diversity as well as pathogens (bacteria, fungus, etc).
SIBO, IMO, and Pelvic Health
So how does this relate to pelvic health? Well, SIBO and IMO are often overlapping issues with pelvic health disorders when it comes to bowel health (constipation & diarrhea), endometriosis, and interstitial cystitis.
- Bowel health. Many people come to pelvic floor PT (PFPT) either on their own or are referred by a physician for constipation and in some instances diarrhea if they have fecal incontinence and leak feces because of weakened or damaged pelvic floor muscles and the surrounding soft tissue. A pelvic floor physical and occupational therapists evaluates and treats outlet disorders which may be due to hypertonic (too tight) or non-relaxing muscles, scar tissue, and pelvic organ prolapse that may be causing obstruction, and muscle strength which can contribute to fecal incontinence. We can also provide some dietary suggestions and have a lot of resources which may be helpful.
- Endometriosis. Research has shown that women with endometriosis are 2.5-5 times more likely to have IBS and gut dysbiosis compared to women without endo. This is true for women who do not have endometriosis found on the bowel (Vigano, Zara, Usai, 2018). Additionally, this is a chronic condition that may contribute to low stomach acid as well as adhesions near or on the intestines. Many people talk about “endo belly” and in addition to swelling around the lesions, this may be one of the causes of abdominal bloating and pain many women with endo describe. For more information on endometriosis watch my webinar here and check out our resource list!
- Interstitial cystitis/painful bladder syndrome (IC/PBS). There has been shown to be an overlap in bladder pain and GI symptoms. There have been thoughts that IC/PBS can be thought of as “leaky bladder” just as GI symptoms can be caused from “leaky gut” or intestinal permeability issues because of inflammation and dysbiosis. Jessica Drummond, MPT, CCN, CHC wrote a blog a couple of years ago that you can read here that goes into depth about the connection between the two and how to treat both. In a study by Weinstock, Klutke, and Lin (2008), 17 of 21 patients diagnosed with IC/PBS also had a positive breath test for SIBO. After antibiotics for SIBO, 73% had moderate to great improvement of their IC/PBS symptoms. This is SO important as we have recently discussed the controversy around IC/PBS in our recent videos which you can find here.
Treatment for SIBO
Treatment of SIBO usually requires the use of either antibiotics, or natural agents can be used as well. Typically antibiotic use consists of Xifaxan +/- an additional antibiotic depending on the result of the breath test. Alternatively, a variety of natural agents can be used. Treatment may last for two to four weeks which is usually followed by a restrictive diet such as the low FODMAP diet to continue to restrict the growth of the bacteria.
A study in 2014 looked at the comparison of the treatment of SIBO with antibiotics versus herbal or natural therapies and showed that both showed a moderate improvement equally. Recommendations included that patients should have a choice between which they prefer and those that were non-responders should attempt to treat SIBO with herbs if they failed antibiotic therapy. Clinically, it is not uncommon to see multiple rounds of treatment to help reduce, or eliminate SIBO treatments.
Updates on SIBO
Recently, Dr. Pimentel has updated the clinical guidelines on all things SIBO and has now distinguished excessive hydrogen vs. methane-producing bacteria. Classically, when there is an overgrowth of bacteria, this is usually related to hydrogen-producing bacteria and is more associated with diarrhea whereas previously methane-dominant SIBO is now named IMO or intestinal methanogen overgrowth as the methane producers are not bacteria, they are classified as archaea. This is an important distinction because they are not bacteria and they require different treatments and clinically present differently. Methane producers usually are more associated with constipation. There is another type that is predominantly hydrogen-sulfide (H2S) producing and can cause issues as well. There are some indications on the breath test that this is what is happening and a classic sign is smelly gas, because it is sulfur gas, so you may notice smelly gas or bowel movements that smell like rotten eggs, this may be what is going on.

As a nutritionist specializing in gut and pelvic health, these are tests that I can offer my clients that I currently work with. To schedule a consultation or get more information you can go to www.pelvicpainrehab.com/nutrition or call 760-487-5118.
References
- Weinstock LB, Klutke CG, Lin HC. Small intestinal bacterial overgrowth in patients with interstitial cystitis and gastrointestinal symptoms. Dig Dis Sci. 2008;53(5):1246-1251. doi:10.1007/s10620-007-0022-z
- Konrad P, Chojnacki J, Gąsiorowska A, Rudnicki C, Kaczka A, Chojnacki C. Therapeutic efficacy of amoxicillin and rifaximin in patients with small intestinal bacterial overgrowth and Helicobacter pylori infection. Prz Gastroenterol. 2018;13(3):213-217. doi:10.5114/pg.2018.74228
- Viganò D, Zara F, Usai P. Irritable bowel syndrome and endometriosis: New insights for old diseases. Digestive And Liver Disease: Official Journal Of The Italian Society Of Gastroenterology And The Italian Association For The Study Of The Liver. 2018;50(3):213-219.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. Am J Gastroenterol. 2020;115(2):165-178.
- Chedid V, Dhalla S, Clarke JO, et al. Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Glob Adv Health Med. 2014;3(3):16-24.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.