
Vulvodynia, Vestibulodynia, and Vaginismus: what’s the difference and why does it matter?
By Stephanie Prendergast, PHRC Cofounder
As many as 28% of women experience painful sex at some point during their reproductive years and that sucks. Knowledge is power and May is Pelvic Pain Awareness Month so we want to provide women with useful information about the three most common diagnoses associated with painful sex: vulvodynia, vaginismus, and vesitbulodynia. Differentiating between these diagnoses is important! Unfortunately these diagnoses are often incorrectly used interchangeably, hindering a woman’s treatment plan. Effective and efficient treatment plans need to be individualized and pelvic floor physical and occupational therapy is almost always a necessary component of a treatment plan for painful sex. While there is some overlap between the vulvodynia, vestibulodynia and vaginismus there are also distinct differences. Let’s break it down.
Basic Definitions
1. Vulvodynia: provoked or unprovoked pain anywhere in the vulva: mons pubis, clitoris, labia majora and labia minora, vestibular bulbs and vulval vestibule, urethra opening, vaginal opening, and Bartholin’s and Skene’s glands.
2. Vaginismus: involuntary pelvic floor contraction that interferes with penetration
3. Vestibulodynia: provoked or unprovoked pain isolated to the vestibule, often characterized by significant redness in this area and tissue atrophy

10 Things you need to know about Vulvodynia, Vestibulodynia, and Vaginismus
- Vulvodynia and vaginismus are also classified as primary or secondary
- Primary vulvodynia or vaginismus: symptoms present from first attempt at penetration
- Secondary vulvodynia or vaginismus: symptoms present after pain-free periods of insertion
- Vaginismus is associated with pelvic floor myalgia (pain) and tightness. A common symptom of vaginismus is vulvovaginal pain which can qualify as a subset of Vulvodynia. However, women with vaginismus can have pain isolated to the pelvic floor muscles and have normal vulvar sensation (no vulvar or vestibule pain) and then this is not technically vulvodynia.
- Studies show that 20 – 90 % of women with vulvodynia and vestibulodynia also have pelvic floor muscle hypertonus/myalgia; since this number is not 100% it is important to note that a percentage of women can have vulvodynia and/or vestibulodynia without having pelvic floor dysfunction. It is more common to have pelvic floor dysfunction and vulvodynia together then to have vulvodynia in isolation.
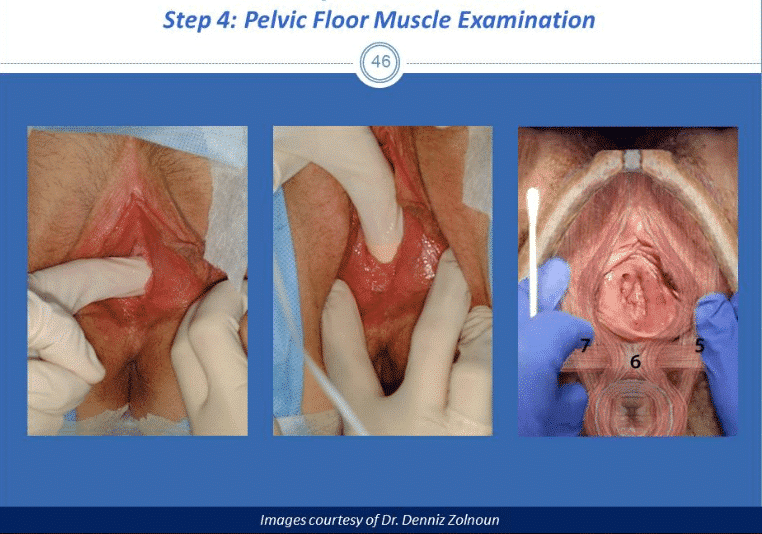
- It is important to perform a visual inspection of the vulva and vestibule for redness (also called erythema) and tissue integrity (or lack of integrity, called atrophy,) and to identify tenderness with the Q-tip test to help determine if the vulva and/or vestibule tissue is involved.
- A pelvic floor physical and occupational therapists is specifically trained to examine the pelvic floor muscles for tenderness, length, strength, and a woman’s ability to voluntarily contract her muscles.
- Visual inspection of the vulva and vestibule, the Q-tip test to the vestibule and vulva, and manual examination of the pelvic floor muscles and vulvar connective tissue will give the provider the needed information to determine which structures are involved.
- Vestibulodynia is a subset of vulvodynia because it involves pain in a specific anatomic vulvar region but excludes pain symptoms in parts of the vulva outside of the vestibule itself.
- The vestibule is a structure sensitive to estrogen and testosterone. Vestibular tissues can become compromised in response to hormonal insufficiencies and if this is the case systemic and topical hormonal therapies may need to be considered to restore tissue health. Hormonal insufficiency can be caused by medications that influence hormones such as oral contraceptive, acne medications, and medications for diseases such as endometriosis. Breastfeeding and menopause affect hormones and therefore also affect the vestibule.
- Not all women with vulvodynia have vestibulodynia. For example, women can have symptoms of vulvodynia characterized only by clitoral pain, interlabial itching, and/or urethral pain. However, many women with vulvodynia also do have pain at the vestibule. If a woman has pain in the vestibule and also the other structures of the vulva it is appropriate to describe the symptoms as vulvodynia and vestibulodynia.
- Vaginismus can exist without vulvodynia or vestibulodynia.
Why the Differential Diagnosis Matters
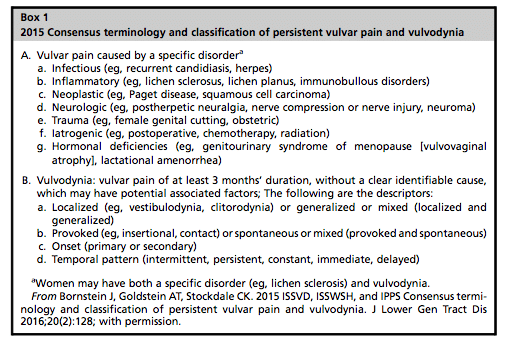
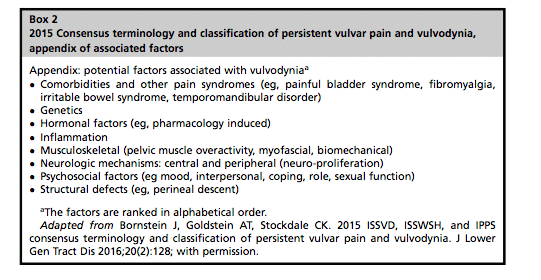
In 2015 the International Society for the Study of Women’s Health, the International Pelvic Pain Society, the International Society for the Study of Vulvovaginal Disease and the National Vulvodynia Association came together to agree on updated vulvodynia terminology to better serve women with these pain disorders. The group was able to conclude from the research that there are seven known causes of vulvar pain and nine associated causes, thereby eliminating the former definition as “idiopathic vulvar pain of unknown cause.”
Thank goodness because it is not reassuring for anyone to have a diagnosis of ‘unknown cause.’ We do know a number of causes of vulvodynia and it’s important that we get all medical professionals up to speed on this.
The consensus publications were a major step forward for women! To read one of the publications please visit the NVA website here. The different causes require different treatments and this is why the diagnostic label matters. Examples are often the easiest way to make sense of this.
Real women, real cases of painful sex:
- Leah is 30 years old. Her vulvar pain developed following multiple urinary tract infections that were appropriately treated with antibiotics but unfortunately led to a number of yeast infections. After her last yeast infection was cleared interlabial itching persisted and intercourse was painful. The evaluation revealed pelvic floor hypertonicity, tenderness and connective tissue changes that were likely caused by infections. She did not have tenderness at the vestibule and did not have vestibulodynia. Musculoskeletal dysfunction, inflammation, and the systemic infections were primary causes of Leah’s vulvar itching and painful sex. Her treatment plan consisted of pelvic floor physical and occupational therapy and medical interventions to stop the urinary tract infection and yeast infections.
- Michelle is 16 years old. Six months ago she began using Accutane for skin issues and was prescribed oral contraceptives as the standard precaution against pregnancy while on this medication. She began to experience insertional pain with tampon use, a symptom she never had before. She bought dilators online to try to treat this symptom and felt persisting pain after each use of the dilators for about 24 hours. Her examination revealed red and fragile vestibular tissues and pelvic floor muscle hypertonus and pain. Her initial treatment plan consisted of stopping the oral contraceptives and acne medication and dilators. Her doctor prescribed her a topical estrogen/testosterone cream. After three weeks of using the cream the tissue was much healthier but she still had pain with insertion, which was confirmed to stem from the pelvic floor muscles. She recovered the rest of the way with pelvic floor physical and occupational therapy and home dilator use. Because her vestibular tissues were initially compromised, any insertion would provoke pain here and therefore the vestibule needed to be treated with topical hormonal medications before pelvic floor physical and occupational therapy and dilators would be therapeutic. The sequence of treatment matters and sometimes certain therapies need to wait until other issues are resolved. Her vestibulodynia was caused by hormonal insufficiencies from both the Accutane and the birth control pills. Sex was painful because of the vestibulodynia, pelvic floor hypertonus, pain and vulvar connective tissue dysfunction.
- Tracey is 18 years old. She tried to engage in sex with her boyfriend and they were unable to achieve penetration. After multiple tries Tracy went to her doctor and the physician had difficulty inserting the speculum due to pelvic floor tightness. They made some progress with a pediatric speculum. Tracy was diagnosed with vaginismus and was referred to pelvic floor physical and occupational therapy and instructed to use vaginal dilators at home. After three months she was able to have pain-free intercourse. Her primary cause of painful sex was musculoskeletal.
Take Home Message
Painful sex is common and very rarely random. Skilled medical providers can almost always find causes and each woman’s treatment should be dictated by the underlying differential diagnosis. If you have painful sex and you are not sure why, a doctor specializing in pelvic pain and a pelvic floor physical and occupational therapists should be able to help! On average, women are misdiagnosed by an average of five to seven providers before finding the help they need. Everyone can help raise awareness by kindly informing past providers of up-to-date information on the topic. One way could be to share the consensus paper.
If you feel like you are stuck in your treatment plan it can be useful to get a second and third opinion from other specialized pelvic floor physical and occupational therapistss and doctors. If you live in the San Francisco Bay area, Los Angeles or New England give us a call, we are happy to help!
How to find doctors and pelvic floor physical and occupational therapistss familiar with pelvic pain
International Society for the Study of Women’s Health
International Pelvic Pain Society
American Physical and Occupational Therapy Association Section on Women’s Health
Herman and Wallace Pelvic Health Institute
Additional Reading
Vulvodynia:
https://pelvicpainrehab.com/category/female-pelvic-pain/vulvodynia-female-pelvic-pain/
Vaginismus:
Vestibulodynia:
https://pelvicpainrehab.com/female-pelvic-pain/3982/jagged-little-pill-part-two/
______________________________________________________________________________________________________________________________________
Are you unable to come see us in person? We offer virtual physical and occupational therapy appointments too!
Due to COVID-19, we understand people may prefer to utilize our services from their homes. We also understand that many people do not have access to pelvic floor physical and occupational therapy and we are here to help! The Pelvic Health and Rehabilitation Center is a multi-city company of highly trained and specialized pelvic floor physical and occupational therapistss committed to helping people optimize their pelvic health and eliminate pelvic pain and dysfunction. We are here for you and ready to help, whether it is in-person or online.
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. The cost for this service is $85.00 per 30 minutes. For more information and to schedule, please visit our digital healthcare page.
In addition to virtual consultation with our physical and occupational therapistss, we also offer integrative health services with Jandra Mueller, DPT, MS. Jandra is a pelvic floor physical and occupational therapists who also has her Master’s degree in Integrative Health and Nutrition. She offers services such as hormone testing via the DUTCH test, comprehensive stool testing for gastrointestinal health concerns, and integrative health coaching and meal planning. For more information about her services and to schedule, please visit our Integrative Health website page.
PHRC is also offering individualized movement sessions, hosted by Karah Charette, DPT. Karah is a pelvic floor physical and occupational therapists at the Berkeley and San Francisco locations. She is certified in classical mat and reformer Pilates, as well as a registered 200 hour Ashtanga Vinyasa yoga teacher. There are 30 min and 60 min sessions options where you can: (1) Consult on what type of Pilates or yoga class would be appropriate to participate in (2) Review ways to modify poses to fit your individual needs and (3) Create a synthesis of your home exercise program into a movement flow. To schedule a 1-on-1 appointment call us at (510) 922-9836
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
I enjoyed reading this article and very helpful information. Thank you for sharing. I recently started my physical therapy practice and offer in specialized treatment of pelvic floor. Hopefully I can help female overcome pelvic pain and dysfunction.
Hello Aman, can you please tell me how do I contact you please? Looking forward..
Hello! You can fill out this form to be contacted https://pelvicpainrehab.com/schedule/