
By: Kim Buonomo, DPT, PHRC Lexington
Who doesn’t love a leisurely bike ride? People with pelvic floor dysfunction! While biking is great cardio, there are a lot of aspects that make it not very pelvic floor friendly. Most of this comes down to blood flow to the pelvic floor, which is what I want to discuss today.
Anatomy Review
In order to understand how biking affects the body, we should review the anatomy. There are a few key areas I think are important to know about: the ischial tuberosities (sit bones), the pudendal neurovascular bundle, and the pubic symphysis (where the pubic bones meet).
Sit down on a firm chair with good posture. Now gently rock yourself side to side. Did you feel the pressure shift from the bony prominence underneath one side of your pelvis to the other? Great! You found your ischial tuberosities or sit bones. This is a common place that we find restrictions in connective tissue and this is one of the places that you get pressure from bike saddles. If you want even more info on connective tissue, you can also check out this article.
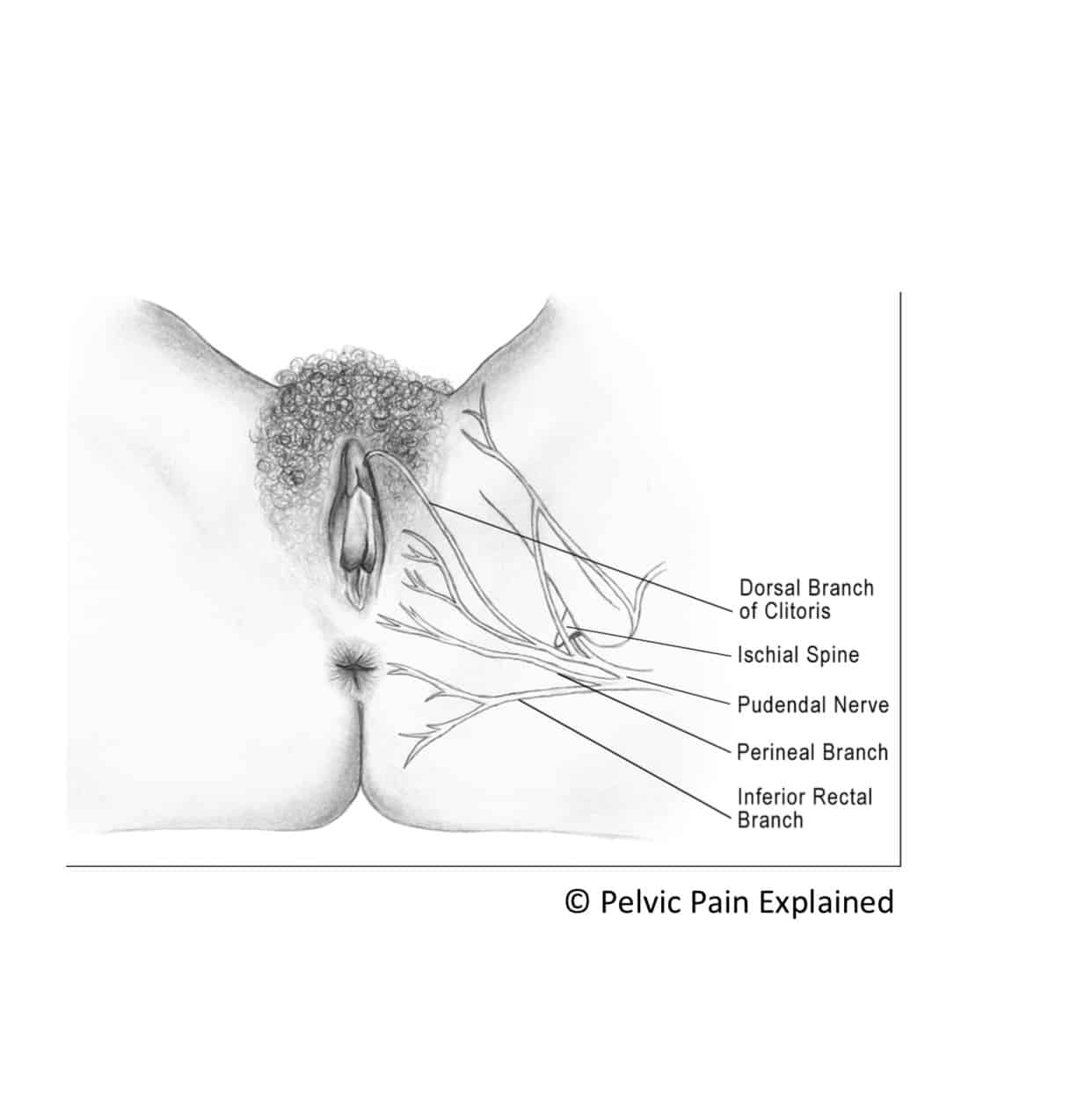
The pudendal neurovascular bundle is a combination of the pudendal nerve, artery and vein. This bundle arises in the sacrum, travels through Alcock’s canal and eventually emerges under the pubic symphysis at the front of the pelvis. The pudendal nerve has three branches and is responsible for sensation to the genitals. It also carries motor fibers to the ischiocavernosus and bulbospongiosus, which are muscles that are important for achieving erection in men and in urinary and sexual function in both sexes.
Pudendal neuralgia is an irritation of the pudendal nerve, which can be caused by many factors, bike riding is one of them. For an excellent overview of pudendal neuralgia, please check out Stephanie’s talk from our Pelvic Pain Explained Webinar Series!
But Kim, what does connective tissue have to do with the pudendal nerve? I’m glad you asked! Connective tissue is the matrix of fascia between our skin and our muscles. We need this matrix to move fluidly in order to avoid pain and restriction. When there is compression or increased strain on the connective tissue (such as sitting on a bike seat) that matrix gets sticky, dense, and can get adhered to surrounding structures (such as the pudendal nerve). The purpose of this increase in tissue density is to protect us from pain and unhealthy movements. When this happens, we find compensations and increased pressure on an already overworked system… which has the potential to lead to conditions like pudendal neuralgia.
Biking and Blood Flow
When it comes to the pelvic floor (or any other part of the body), one of the most important factors to consider is blood flow. Good blood supply is crucial for normal function, and when muscles or nerves do not have adequate blood flow, they get cranky. Think about when you get your blood pressure taken and the cuff stays on your arm for just a little too long. The part of your arm below the cuff might start to tingle or feel uncomfortable. You may have difficulty moving your hand until the pressure is taken off and blood flow is restored. When you compress your pelvis under a bike saddle, a similar phenomenon is happening.
Pelvic floor symptoms such as perineal pain, tenderness, numbness, and sexual dysfunction are all believed to be caused by compression of the pudendal neurovascular bundle where it arises under the pubic bone at the pubic symphysis. Increased pressure from sitting on a bike saddle is also associated with urological dysfunction, erectile dysfunction, and genital and perineal discomfort. In short, a lot of bad things for the pelvic floor, but also a lot of things PT can address. If you have any of these symptoms, make an appointment with one of our offices for an evaluation. All of our therapists are skilled in the management of pelvic pain!
Bike Seats
There are many options of bike saddle available to today’s riders. Many different saddle variations have been studied to determine how this impacts the pelvic floor.
One study compared four different saddle types and their impact on penile oxygen supply. While this study only had male participants, it can be generalized to female riders, who also often report pelvic symptoms from bike riding.
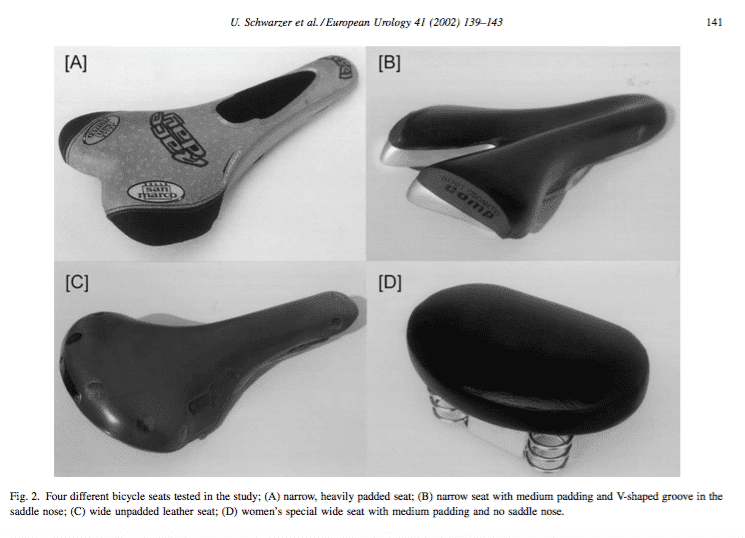
Image courtesy of: Schwarzer, Sommer, Klotz, Cremer and Engelmann. Cycling and Penile Oxygen Pressure. European Urology. 41.139-143. (2002)
The results were interesting. After 20 minutes of riding at 60-65% of the participant’s heart rate maximum, there was a significant decrease in penile oxygen pressure in all riders. With the narrow, heavily padded saddle, penile oxygen decreased by 82.4%. With the narrow, less padded saddle, it was 72.4%. With the wide, unpadded seat, it was 63.3% and the noseless saddle was 20.3%.
Let me say that again… Even the best saddle in this study decreased penile oxygen by 20% in as little as 20 minutes!
That’s a pretty significant decrease, and can make the pelvic floor pretty grumpy!
Risk factors for pudendal neuralgias and paresthesias from biking include poor bike fit, increased time in the saddle, minimal position change and increased body weight. A wider saddle did seem to help increase comfort and decrease pelvic symptoms in participants surveyed. Increased saddle pressure was also found in cyclists with a lower handlebar position. This makes sense, as a lower handlebar means that you are leaning more forward and putting more pressure onto the perineum, compressing the pudendal neurovascular bundle against the pubic bone at a greater degree. Lower handlebar position was also associated with decreased sensation in several critical pelvic floor structures in women (again, I feel that these results are easily generalized to include anyone sitting on a bike saddle).
An important point to remember is that the studies I’m writing about took place in a lab on a stationary bike. Riding on real roads, paths, and trails can lead to real bumps, potholes and uneven terrain that your pelvic floor may not love. Also, you need to shift your body weight as you ride, which affects the rest of your pelvic girdle and can contribute to blunt trauma to the perineum and increased pelvic floor damage over time.
So why can some people ride bikes and be perfectly fine while others develop symptoms? In a way, this comes down to individual differences between people. When any body part exceeds the workload that it is capable of, things can become sensitized and irritated. Different people with different body shapes, sizes, physical activity history, and body compositions will have different capabilities of their tissues, and some people may be able to ride bikes all they want and stay below the “overworked” threshold. Others may tolerate riding for years before their tissues show signs that they have become overworked. And for some people, riding even short distances may be too much. Differences in the shape of the pelvis and the soft tissues surrounding the ischial tuberosities can also impact your weight distribution, which impacts how these structures are compressed on the saddle and how the connective tissue compensates. Studies report that 7-8% of cyclists on long distance rides experience penile or labial numbness, and other studies report the prevalence to be as high as 50% to 91%!
I have symptoms. What can I do about it?
- Take a break from cycling
Have you ever heard the joke where the patient says “Doctor! It hurts when I do this.” And the doctor says, “Well, don’t do that!” We never want our patients to give up something they love, and one of our goals is always getting you back to pain free activity. But that said, there are benefits to giving your pelvic floor a chance to rest and recover from periods of increased strain and decreased blood flow. Your body is designed to heal itself, but we have to help set it up for success. So, if possible, switching to walking or swimming can be a great way to maintain fitness without that prolonged pressure on your pelvic floor.
- Stand up!
If giving up cycling completely is not an option, make sure to change your riding position frequently. This limits long term compression and deflates the blood pressure cuff from my earlier analogy. There isn’t firm research for how frequently you should change your position, but a good rule of thumb is standing for 30-60 seconds for every 10 minutes of riding.
- Pick your saddle wisely
Think about the study I mentioned above. The difference between the “best” saddle and the “worst” saddle was over 60% as measured by percentage of oxygen change. There is no arguing that modifying the saddle made an impact here! Generally, you want a saddle that is wide, so your weight is evenly distributed on your ischial tuberosities, which are better designed to absorb and redistribute that pressure. The angle of your pelvis on the seat is also important (I’ll talk about that next). You should always see a professional to get your bike seat properly fitted. Broader saddles are associated with a significantly lower rate of saddle related symptoms in female riders, as well as more comfort during a bike ride.
- Think about your pelvic posture
We talk about pelvic position and posture a lot on this blog. Studies have shown a decrease in the available space under the pubic symphysis when a rider goes from an upright sitting position to an anterior pelvic tilt, such as when leaning forward over low handlebars. With less space under the pubic symphysis, there is less space for the artery and nerve and greater likelihood for something to be compressed. Higher handlebars may help improve upright sitting position and decrease anterior pelvic tilt.
Biking is a dynamic activity that engages your arms, core, hips, legs, and pelvis, and balances all of that on two wheels. And who better to assess all of these moving parts than a movement specialist! There is a lot more information out there about biking and low back pain, pelvic pain, glute weakness, and more. If you are having any symptoms that you think may be related to bike riding, see a PT like me for an assessment!
______________________________________________________________________________________________________________________________________
Are you unable to come see us in person? We offer virtual appointments!
Due to COVID-19, we understand people may prefer to utilize our services from their homes. We also understand that many people do not have access to pelvic floor physical and occupational therapy and we are here to help! The Pelvic Health and Rehabilitation Center is a multi-city company of highly trained and specialized pelvic floor physical and occupational therapistss committed to helping people optimize their pelvic health and eliminate pelvic pain and dysfunction. We are here for you and ready to help, whether it is in-person or online.
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. The cost for this service is $75.00 per 30 minutes. For more information and to schedule, please visit our digital healthcare page.
In addition to virtual consultation with our physical and occupational therapistss, we also offer integrative health services with Jandra Mueller, DPT, MS. Jandra is a pelvic floor physical and occupational therapists who also has her Master’s degree in Integrative Health and Nutrition. She offers services such as hormone testing via the DUTCH test, comprehensive stool testing for gastrointestinal health concerns, and integrative health coaching and meal planning. For more information about her services and to schedule, please visit our Integrative Health website page.
References
- Trofaier, Marie-Louise; Schneidinger, Cora; Marschalek, Julian; Hanzal, Engelbert; Umek, Wolfgang. “Pelvic floor symptoms in female cyclists and possible remedies: a narrative review.” Int Urogynecol J. 27,513-519. (2016) doi:10.1007/s00192-015-2803-9
- Larsen AS; Larsen FG1; Sørensen FF; Hedegaard M; Støttrup N; Hansen EA1; Madeleine P. “The effect of saddle nose width and cutout on saddle pressure distribution and perceived discomfort in women during ergometer cycling.” Appl Ergon. Jul;70:175-181. (2018) doi: 10.1016/j.apergo.2018.03.002.
- Schwarzer; Sommer; Klotz; Cremer; Engelmann. “Cycling and Penile Oxygen Pressure.” European Urology. 41.139-143. (2002)
- Kotler D; Babu A; Robidoux G. “Prevention, Evaluation, and Rehabilitation of Cycling-Related Injury.” Current Sports Medicine Reports. Training, Prevention, and Rehabilitation. 15 (3). May/June (2016)
- Asplund C; Barkdull T; Weiss B. “Genitourinary Problems in Bicyclists” Current Sports Medicine Reports. 6:333-339 (2007)
- Leibovitch I; Mor Y. “The vicious cycling: bicycling related urogenital disorders” European Urology. 47:277-287. (2005).
- Gemery JM; Nangia AK; Mamourian AC; Reid SK. “Digital three-dimensional modelling of the male pelvis and bicycle seats: impact of rider position and seat design on potential penile hypoxia and erectile dysfunction.” BJU Int. Jan;99(1):135-40. (2007)
- Rodseth M; Stewart A. “Factors associated with lumbo-pelvic pain in recreational cyclists.” South African Journal of Sports Medicine. 29:1. (2017)
- Bressel E; Larson BJ.“Bicycle seat designs and their effect on pelvic angle, trunk angle, and comfort.” Med Sci Sports Exerc. Feb;35(2):327-32. (2003)
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
Thank you, very helpful info. I have strained my pelvic floor muscles when I had crossed a few overpasses every time during my cycling. Now I’m doing Kegel exercises and don’t cycle but I would like to. I’m interested how long it takeS to recover?
Thank you again
Irena
Hi Irena,
Recovery is different for everyone. This can depend on your current state of your pelvic health and your treatment plan for recovery (if you have one). Have you reached out to a pelvic floor PT recently to help assist in recovery? They can help evaluate where you are at now, in order to be most effective in your recovery.
Regards,
Emily
Hi, Dr. Buonomo. This article hits close to home. Thanks so much for posting it. I first started experiencing pelvic pain in Jan 2019. The good news is, my symptoms have cleared up dramatically with pelvic floor PT. One thing that continues to trigger some pain and discomfort is a hard interval workout on my road bike. I am certain it comes from rolling my pelvis into the nose of the bike seat. I think I could solve or reduce my problem by finding a bike seat with a larger cutout. Can you recommend a bike seat with a large cutout? I have been looking at models from Selle Italia and ISM. Once again, thank you for the article.
Hi Mark,
While a new seat may be helpful, we highly encourage you to get a good bike fit before changing your saddle, as that can make as much if not more of a difference in saddle comfort. Nose pressure (or rolling forward) in your seat may be tilted anteriorly and causing you to roll forward onto the nose of the saddle and leading to discomfort and pressure on the soft tissues in the pelvic floor. We would like to refer you over to Curtis and Justin. They work with Revolution Fitness, and are offering video fits for 30 minutes and may be able to help you, even if you are not in this area. Overall, our experiences thus far has really taught us that a good bike fit is the best place to start.
Here is the link directly to their video fit page: https://revolutionsinfitness.com/video-fit-consultation