
By Admin
“In all nature structure determines function” – William Herbert Sheldon, father of somatotyping
“Form and function are a unity, two sides of a coin” – Ida P. Rolf, biochemist and fascial genius
“Conjunction junction, what’s your function?” – Schoolhouse Rock, how us 30+s learnt grammar
Structure and function are intricately connected. Our posture is the structure in which we move and function in the world. For example, when our ancestral primates chose to become bipedal, the hip joint changed to allow for increased mobility and centered weight bearing. For a more present day example look no further than your smart phone. Yes, that little device has created quite a number of neck and upper body problems, leading to what health care professionals like to call “text-neck.” Side note: Did you know that just a 15 degree bend in your neck to look down at your phone more than doubles the weight of your head. Physics people- no wonder your neck is tight. If you’re reading this right now on your smart device just lift up the phone to eye level and see the difference in effort for those neck and upper back muscles. Ok, stepping off my soapbox now. Basically, how we use our bodies impacts how our bodies form. And the form of our bodies impacts what we can and cannot do. My personal journey with posture has been one from ignorance, to militantism, to defeat, and now to hope. I spent a long time trying to “correct” my posture by “standing up straight” and “sucking in my gut,” as my mom used to tell me. Ultimately, I just resigned myself to the fact that I lacked enough strength and motivation. But now I know better.
Posture is not a position you hold, but rather a state of balance.
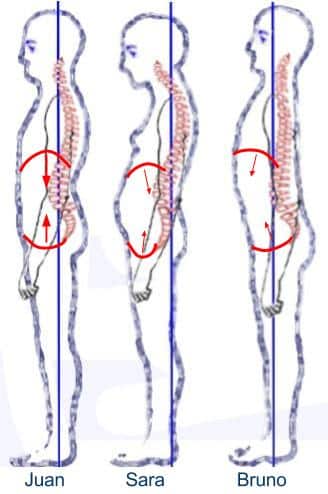
Let’s take a look at our friends, Jaun, Sara and Bruno to explain it better.

At first glance, who seems most balanced? Sara looks like she may be developing some of that text-neck and possibly back pain. Bruno is trying really hard to stand up straight. He may eventually get tired, or just live with constant discomfort and tightness in his upper back. Now Juan, he’s not perfect, but I think out of the group he seems most balanced and comfortable. I have a disclaimer: not all people named Juan, Sara and Bruno stand like this. Not all ladies are Saras and not all gentlemen are either Bruno or Juan. These postures are not the only postures out there. This is a google image for educational purposes. Ok, so back to the picture. What else indicates that Juan’s muscles and joints may have less stress on them? This is where we go back to the books to explore what us professionals like to call base of support and alignment. Juan is stacked up over his base of support (feet) and has reasonable alignment. He’s a little extended in his ribcage- but again, google image. Overall, his pelvis is over his feet, his ribcage is over his pelvis and his head is over ribcage. Sara does not have efficient alignment. Her ribcage is behind her pelvis and her head is in front of her ribcage. And Bruno…well Bruno’s ribcage is already into next week leaving his pelvis and head behind to catch up. Now let’s finally get to the point of the blog: how posture impacts our muscles, specifically our pelvic floor. To demonstrate my point I’ll show you the same picture with the pelvic floor and diaphragm (basically the “thoracic floor”), drawn in.

Okay, I know it’s a little rough, but hopefully you can see what I mean about Juan’s base of support and alignment. His diaphragm (the top red arc), is lined up over his pelvic floor (the bottom red arc). For Sara and Bruno the arcs are not stacked over one another, and there are even some changes in muscle length and shape. When the ideal length-tension ratio of a muscle is changed, it can’t function as well and this leads to weakness. What’s more, the pelvic floor and the diaphragm, along with some other trunk muscles, are part of the “core.” So when the “core” can’t fire efficiently, dysfunctional movement patterns develop that can create pain. To help explain this a bit better, I have one more picture to show the “strength” and direction of the pelvic floor and diaphragm in each position. (Bigger arrows mean more force/pressure production because of better length/tension of the muscle).
So who’s got the the big arrows? Juan! Sara and Bruno just can’t catch a break. Their muscles cannot produce as much force as Juan’s and don’t work together as well. The primary role of the core muscles is to increase intra-abdominal pressure (IAP) in order to keep the trunk stable. For a basic idea think: floppy balloon versus blown up balloon- which is easier to deform? Of course, the body’s balloon has active muscular walls and the top of the balloon (diaphragm) keeps letting air in and out for breathing, but the general premise is accurate. The great thing about our body is its structure is built for this function- to automatically turn the “core” on when we are in an efficient alignment. Think of how babies grow into toddlers and then into children who run, walk, sit efficiently, and with no pain. No one told them how to do that, their bodies automatically learned from guess and test and retest. Sometimes, after pain our muscles do get inhibited and we need to cognitively turn them on, but often changing to a more efficient posture can actually provide the same or even better strength gains.
So this is all great, but how does it apply to real life scenarios. Well, let’s imagine Sara is one year postpartum and came into the clinic because of incontinence. She’s trying to get back to exercise, but feels like she’s weaker than before she gave birth and is “leaking a little” with her box jumps. She may have even been doing her kegels correctly, but she still can’t get over that hurdle. Perhaps, it’s not as much an issue with strength, but more a problem with her alignment. She actually is weaker than before. Before getting pregnant, she was a Juan-like, but after pregnancy, birth and running around taking care of a one year old, that whole posture-thing fell to the wayside. She also may be a teensy-bit stressed leading to shallow breathing and decreased use of her diaphragm- another core muscle. Recent research out of Australia has even linked breathing capacity to incontinence, back pain and GI distress. To see just the impact breathing can have on stress and your bathroom habits check out Nicole’s blog. Since we understand the mechanics of the core and posture a bit better, this isn’t too surprising.
But remember, your pelvic floor muscles can also be too tight because of postural holding patterns. Maybe Sara actually shortened her pelvic floor muscles from doing so many kegels and now it’s not slack but like a tightrope. Maybe Bruno has started taking a lot of crossfit classes and is really working on “standing up straight,” but also noticed since signing up for his monthly membership, it takes him a while to start urinating and ejaculation has become painful. Normalizing posture, by aligning the body over the base of support can help improve the efficiency of the pelvic floor and diaphragm, so the muscles don’t have to work as hard. And when the muscles chill out, then the pain will start to dissipate. Take a look at some other exercises that can help improve the mobility of the pelvic floor. Often, if the muscles have been short for a while they also may need manual work, that’s where the PHRC or any good pelvic floor PT comes in.
So this is a lot to digest in one sitting. Hopefully you are still reading your phone at eye level and haven’t dropped it back in your lap. We’ll have a Posture and the Pelvis: Part Two to teach you how to apply these concepts to your own body. But please, don’t wait with bated breath. Just keep that diaphragm moving in the meantime.
______________________________________________________________________________________________________________________________________
Are you unable to come see us in person? We offer virtual appointments!
Due to COVID-19, we understand people may prefer to utilize our services from their homes. We also understand that many people do not have access to pelvic floor physical and occupational therapy and we are here to help! The Pelvic Health and Rehabilitation Center is a multi-city company of highly trained and specialized pelvic floor physical and occupational therapistss committed to helping people optimize their pelvic health and eliminate pelvic pain and dysfunction. We are here for you and ready to help, whether it is in-person or online.
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. The cost for this service is $75.00 per 30 minutes. For more information and to schedule, please visit our digital healthcare page.
In addition to virtual consultation with our physical and occupational therapistss, we also offer integrative health services with Jandra Mueller, DPT, MS. Jandra is a pelvic floor physical and occupational therapists who also has her Master’s degree in Integrative Health and Nutrition. She offers services such as hormone testing via the DUTCH test, comprehensive stool testing for gastrointestinal health concerns, and integrative health coaching and meal planning. For more information about her services and to schedule, please visit our Integrative Health website page.
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.
Comments
Thanks for the great post. For a lot of folks its hard to even hear the word posture without rolling their eyes and conjuring up memories of feeling nagged. Unfortunately, a lot of providers adopt similar pessimistic attitudes about getting their patients/clients to change the way they hold their bodies during all those hours when they are not in treatment. I look forward to reading and sharing Part Two.