By Kim Buonomo, DPT, PHRC Lexington
Many women do not realize how common pelvic floor dysfunction is after giving birth. We often hear patients who think it is normal to leak urine or to be unable to exercise after having children. Postpartum pain is common, but not normal, and pelvic floor physical and occupational therapy including pelvic floor muscle contraction exercises is recommended to treat persistent urinary incontinence postpartum, regardless of the type of incontinence. When symptoms occur postpartum, pelvic floor therapy can help to “rewire” the brain and muscles to control the coordination of key muscle groups. Pelvic floor therapy can be used to address a variety of conditions that are common after pregnancy such as:
- Urinary incontinence & frequent urination, including frequent nightly urination
- Overactive bladder
- Stress incontinence
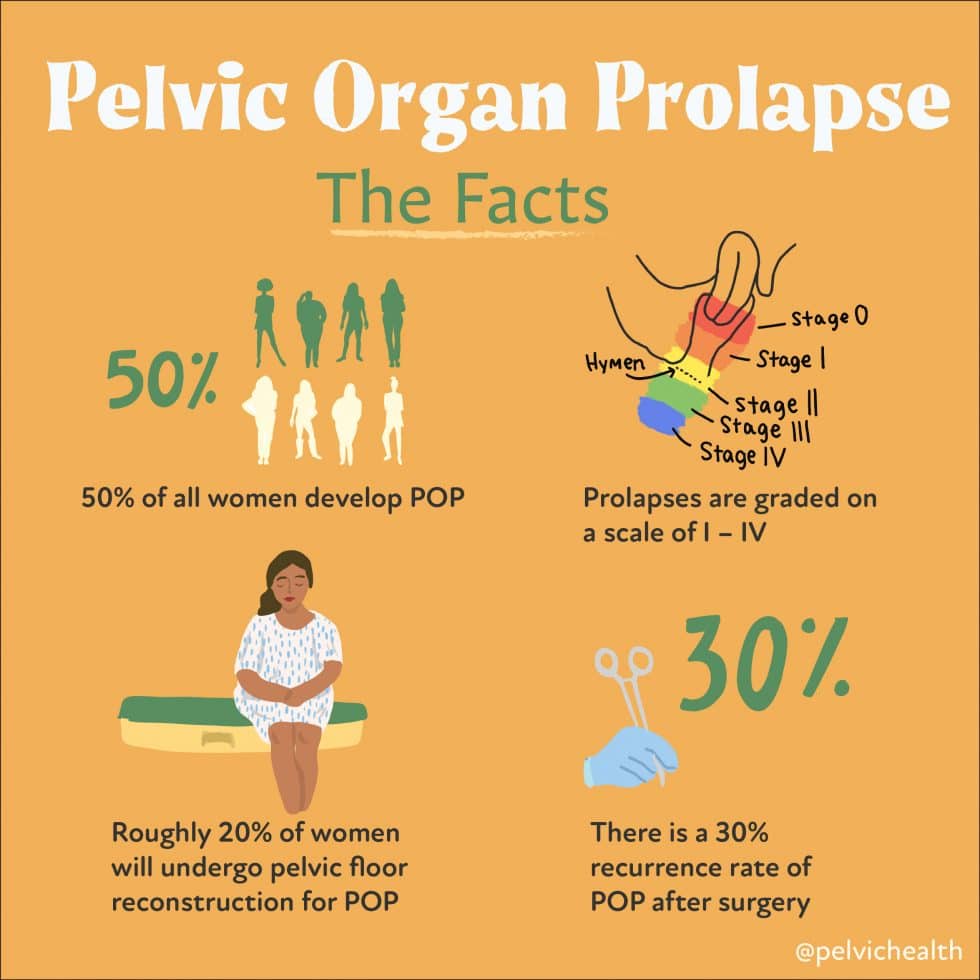
- Pelvic organ prolapse
- Fecal incontinence
- Chronic constipation
And so much more!
Today, I’m going to tell you how we helped Jamie recover after giving birth to her first baby.
Her Story
Jamie gave birth to her first baby in August of 2019. During delivery, she pushed for an hour and a half and had two tears which required stitches. She did not require vacuum assist or the use of forceps to deliver. She came to me in October 2019 (10 weeks after delivery). She had strained during a bowel movement about a month after giving birth, and ever since, she reports being able to see and feel a prolapse (heaviness, and internal tissue descending from the vaginal opening.) Her OBGYN told her that this was normal, but did not provide any options for relief, so she went to a urogynecologist who gave her a pessary. She reports that the pessary seemed to help when it was in, but she was bleeding and had pain during removal of the pessary.
Jamie had limited ability to participate in exercise due to her symptoms. She had a feeling of heaviness in the pelvis like a tampon sticking halfway out. Here is a summary of the symptoms she reported to me.
Urinary symptoms: post void dribble, urinary urgency, weak stream, sometimes needing to strain to get the last bit of urine out.
Bowel symptoms: chronic constipation, using squatty potty which helps. Hemorrhoids during pregnancy and after delivery. Rectal pressure with bowel movements.
Sexual symptoms: has not returned to sex since giving birth, and is concerned about her return to sexual activity. Due to the bleeding she had with pessary removal, her gynecologist started her on a topical estrogen.
Jamie had seen two other physical and occupational therapistss before coming to our clinic, and was not satisfied with the quality of care she received, so she found us online and after researching us a bit, knew that we were the providers she wanted on her team.
Assessment
My evaluation showed a grade two cystocele (anterior wall prolapse), pelvic floor weakness, diastasis recti (a separation of the rectus abdominis or “six pack” muscle), muscular restrictions of the urogenital triangle (the superficial muscles responsible for urinary and sexual function… this is the muscle group that tore during her delivery), irritation and erythema of the vestibule (redness of the entryway to the vagina), and positive active straight leg raise test. She didn’t have any connective tissue dysfunction. This made me think that after giving birth and the tearing she experienced during delivery, her pelvic floor became weak, which meant that it was less able to support itself. Given her history of chronic constipation, I thought that straining during the particularly difficult bowel movement a month after delivery was “the straw that broke the camel’s back” and pushed her prolapse to the point where it was now noticeable to her. Here is my mental breakdown of her symptoms and the most likely contributing factors:
- We know that the two biggest contributors to prolapse are vaginal delivery and constipation/straining due to the increase in pressure in the abdomen pushing down on the pelvic floor. Both of these risk factors are in her recent medical history, so it makes sense that she would be more susceptible to prolapse. Prolapse often causes the feeling of heaviness, or a tampon sticking out of the vagina like Jamie reported.
- Weakness of the pelvic floor muscles, which is very common after a vaginal delivery, contributes to the insufficiency of these muscles to respond appropriately to increased intraabdominal pressure with lifting and moving. The fact that she had vaginal tearing during delivery means that the muscles were damaged. This can cause tightness and muscle guarding of the pelvic floor muscles and can contribute to her feeling of heaviness or prolapse. One way to decrease risk of tearing is perineal massage! I encourage all of my patients who are planning to have a vaginal delivery to perform perineal massage for the six weeks leading up to delivery (starting at 34 weeks of pregnancy).
- She had signs of hormone dysfunction, including the erythema or redness of her vestibule, reports of abnormal bleeding with removal of the pessary, and vaginal dryness. In lactating women estradiol levels remain low as long as prolactin levels remain high. While these changes are typical for a newly postpartum and still lactating woman, we also know that lack of estrogen can contribute to symptoms of vestibulodynia, as we see with patients who take oral contraceptives, or who are postmenopausal. I suspected that her hormone fluctuations were playing a role in her pelvic floor symptoms.
- The active straight leg raise test showed weakness of the transverse abdominis (one of your major core muscles). Again, I would expect to see this postpartum, since pregnancy affects three of the four anticipatory postural muscles, including TA. We know that the TA also plays a big role in supporting the internal canister and maintaining pressure. When this pressure escapes through the pelvic floor, it can be another factor that contributes to symptoms of prolapse.
- Diastasis recti is another common condition with pregnancy and postpartum. The rectus abdominis is your six pack. The six pack muscle is separated into two halves that are connected by fascia called the linea alba. Many conditions can make someone more susceptible to diastasis. These include history of abdominal surgery, significant fluctuations in weight, pregnancy/postpartum, and chronic constipation/straining. Similar to prolapse, this condition is also influenced by intra abdominal pressure.
My goals for Jamie
Short Term (four to eight weeks):
Will demonstrate closure of the diastasis recti.
Will demonstrate improved pelvic floor contraction to grade four out of five.
Long Term (eight to twelve weeks):
Will report improved tolerance to activities of daily living including light exercise without feeling of prolapse.
Will return to intercourse with minimal discomfort.
Plan
All in all, Jamie’s presentation made a lot of sense. She had some of the classic symptoms of pelvic organ prolapse and we know this is a common condition which affects 41-50% of women examined in the USA. She also had risk factors in her history which include vaginal delivery and constipation. She only delivered 10 weeks prior to her evaluation, so I knew that some healing would come with time… I like to tell my postpartum patients that if it took nine months to grow the baby, you should give yourself nine months to recover. However, there are many patients who feel great weeks after delivery, and there are also many patients who are still working to achieve their goals for a year. This is a really individual process. Ultimately, we came up with a plan to help her recovery go as smoothly as possible.
The main components of this plan were:
- Managing her intra-abdominal pressure.
I believe prolapse management is just as much about avoiding the wrong things, as it is about doing the right things. When we strain like the valsalva maneuver -with constipation, childbearing, ineffective lifting mechanics, exercises that increase pressure in the abdomen, or anything that asks you to bear down- this increases the pressure in the abdomen. When that pressure isn’t being managed effectively, it has to go somewhere. Think about it this way: If you had a can of soda which is being “effectively managed”, ie: the can is intact, the seal isn’t broken, etc. you could shake up the can without anything bad happening. When the can is not being “effectively managed”, ie: has a hole in it, someone crushed the sides, popped the top, etc. and you shake up the can… bad things happen. In the human body, this could mean urine leakage, symptoms of prolapse, etc. For more about this concept, check out this blog article!
In order to work on this concept, we focused on making sure she had good posture and was engaging her core muscles effectively. I also wanted to make sure she understood the movements of her pelvic floor and could use those muscles effectively, meaning, drop instead of strain. We reviewed body mechanics with posture, lifting, and all the activities I mentioned above.
- Strengthening her pelvic floor muscles
Vaginal delivery is a trauma to the pelvic floor muscles, and we knew that those muscles were torn/damaged during delivery. She had weakness of the pelvic floor, and strengthening these muscles in the right way helps them to support the inner vaginal wall. Physical therapy has been shown to decrease pelvic organ prolapse by up to one grade.
- Working with the rest of the medical team.
Her urogynecologist was a critical team member. Jamie showed signs of low estrogen, which were treated with a topical estradiol. Her gynecologist also went through the process of fitting her with a pessary. It can take multiple attempts to find the pessary which is most comfortable for the patient, but up to 75% of women can be fit effectively. Jamie had to try a few different pessary options before finding the solution which supported her best, and her urogynecologist was instrumental in that process.
Success!!
- Describe the patient hitting their goals, and any insight into what you think made the biggest difference.
Jamie did really well with physical and occupational therapy. We know that healing takes time. For muscle strengthening, it often takes about six to eight weeks to notice a change. Jamie started to see progress at her seventh week of physical and occupational therapy, which is exactly what we would expect. At that time, she noted that the vaginal pressure had improved, but she was still having rectal pressure. Three weeks later, the rectal pressure was also improving. Jamie was always asking questions and having me check her form with exercise, and she understood how important it is to move effectively. I believe that was a big factor for her to understand how to keep herself well to avoid exacerbating the prolapse. She did have a setback when she had a cold and was coughing a lot, so she relied on the pessary more often and seems to have more heaviness in the following weeks. It is possible that this prolonged her time of care at PHRC. I saw her for about four months in total. Even though she had a long road, Jamie ended up doing really well and is now pregnant with her second baby!
Here are her thoughts on her PT experience: “I visited PHRC after working with two other therapists. Having a background in Exercise Science, I was eager to find someone who was willing to help me achieve my goals of returning to activity through education and hands-on work. Kim did both of those things. We discussed both my and her short- and long-term goals, along with an action plan to achieve those goals. Kim had to slow me down (mentally and physically) to allow my body time to heal. My time spent with her involved lots of manual work, but also mental re-training and slowing down to focus on the little things, like breathing. I had my ups and downs, but ultimately grew stronger, less symptomatic and was able to gradually return to phased activities, which now include, biking, running, lifting weights, yoga and all physical activities with my toddler boy. I also was able to resume pain-free intercourse, and Kim was also my biggest cheerleader and guide to everything intercourse-related. I am now halfway through my 2nd pregnancy, and re-consulting with Kim on how I can have a safe pregnancy, labor and delivery. I wish all women had the chance to be educated on the pelvic floor BEFORE sustaining an injury. However, it’s never too late and there are very well-trained professionals who can help return to a new sense of normalcy.”
Did physical and occupational therapy help you with your prolapse? Tell us about it in the comments!
If you suspect that you may have prolapse, physical and occupational therapy can help! Contact one of our offices or request a digital health appointment today!
References
Physical and Occupational Therapy for Incontinence, Prolapse and the Pelvic Floor
Deffieux X, Vieillefosse S, Billecocq S, Battut A, Nizard J, Coulm B, Thubert T. Rééducation périnéale et abdominale dans le post-partum: recommandations [Postpartum pelvic floor muscle training and abdominal rehabilitation: Guidelines]. J Gynecol Obstet Biol Reprod (Paris). 2015 Dec;44(10):1141-6. French. doi: 10.1016/j.jgyn.2015.09.023. Epub 2015 Oct 31. PMID: 26530172.
>
McNeilly AS. Effects of lactation on fertility. Br Med Bull. 1979 May;35(2):151-4. doi: 10.1093/oxfordjournals.bmb.a071562. PMID: 387162.
American College of Obstetricians and Gynecologists (ACOG). (2007). Pelvic organ prolapse. ACOG Practice Bulletin No. 85. 110, 717-729
Atnip, S., & O’Dell, K. (2012). Vaginal support pessaries: Indications for use and fitting strategies. Urologic Nursing, 32(3), 114-125.
______________________________________________________________________________________________________________________________________
Are you unable to come see us in person? We offer virtual physical and occupational therapy appointments too!
Due to COVID-19, we understand people may prefer to utilize our services from their homes. We also understand that many people do not have access to pelvic floor physical and occupational therapy and we are here to help! The Pelvic Health and Rehabilitation Center is a multi-city company of highly trained and specialized pelvic floor physical and occupational therapistss committed to helping people optimize their pelvic health and eliminate pelvic pain and dysfunction. We are here for you and ready to help, whether it is in-person or online.
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
In addition to virtual consultation with our physical and occupational therapistss, we also offer integrative health services with Jandra Mueller, DPT, MS. Jandra is a pelvic floor physical and occupational therapists who also has her Master’s degree in Integrative Health and Nutrition. She offers services such as hormone testing via the DUTCH test, comprehensive stool testing for gastrointestinal health concerns, and integrative health coaching and meal planning. For more information about her services and to schedule, please visit our Integrative Health website page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Like us on Facebook,
Subscribe to our YouTube Channel,
and follow us on Twitter, Instagram, Tik Tok and Pinterest!
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.