
By Stephanie Prendergast, MPT, Cofounder, PHRC West Los Angeles
A frequent question from social media:
“I have Vestibulodynia and painful bladder syndrome. I am almost symptom free except for near or during my period. My hormone levels are fine. My urologist prescribed testosterone cream because he found atrophy. At the same time I have another doctor telling me that to reduce inflammation caused by the hormonal variations of the period I should take continuous birth control pills, which I heard can make things worse. I appreciate any insight that you can offer.”
The Answer:
Are oral contraceptive pills a cause of pelvic pain or are they a solution? Questions like the one above come up frequently, and part of the problem is defining ‘pelvic pain.’ By current usage, the term ‘pelvic pain ’encompasses a number of symptoms: menstrual cramps, vulvar pain, painful sex, and irritative bladder symptoms. These symptoms have different causes and different treatments, by narrowing the definitions we can better answer the above question.
Pelvic Pain: vulvar pain and irritative bladder symptoms
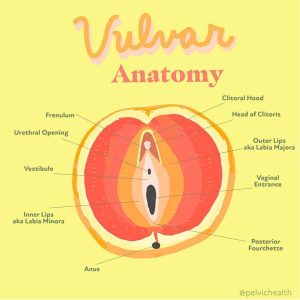
The vulvar vestibule and the urethra and bladder are derived from the same embryological layer: the intermediate mesoderm urogenital sinus. There are a number of reasons why people often have symptoms of both Vulvodynia/Vestibulodynia and painful bladder syndrome/Interstitial cystitis, and the fact they share an embryologic layer is one of them. A second reason is because the vestibule, urethra and bladder are hormonally sensitive structures. In order for these organs to function normally they need estrogen and testosterone, hormone insufficiency affects the bladder and the vulva. A third reason why people often feel both irritative bladder symptoms and vulvar pain is because of their close proximity to the pelvic floor muscles. Numerous research studies show that the majority of patients with Vestibulodynia/Vulvodynia and irritative bladder symptoms also have pelvic floor dysfunction.
Research has shown that some women will develop Vestibulodynia from taking oral contraceptive birth control pills. If women start birth control pills under the age of 17 there is an 11-fold risk of developing this syndrome, in women over the age of 17 there is a 4-fold risk. Certain people have a genetic polymorphism, meaning specific properties in their DNA, that are more likely to become compromised than others by reduced circulating free testosterone and elevated SHBG. These are two of the changes that occur when taking OCPs. Please note, when we are discussing hormonal deficiencies in premenopausal women we are not talking about estrogens which require testing at specific points in the menstrual cycle. These tests often return ‘normal’ or ‘fine, and not the main reason people are symptomatic. The majority of physicians do not test for SHBG and may not calculate a person’s free testosterone.
For more information about the exact mechanisms check out:
Do Oral Contraceptives Cause Vulvodynia
Jagged Little Pill Part One and Part Two.
Pelvic Pain: Dysmenorrhea (menstrual cramps)
Anyone who has a period knows that oral contraceptives are offered as solutions for everything: reducing menstrual flow and length of menses, to help acne, to ‘regulate’ periods, and to reduce dysmenorrhea (painful cramps). When most general gynecologists hear ‘pelvic pain’ they usually think of Dysmenorrhea. Dysmenorrhea is a common symptom of Endometriosis, and this doctor may or may not know much about Vulvodynia or Interstitial Cystitis. Research shows that oral contraceptive pills will lessen the symptom of dysmenorrhea. These pills do not treat endometriosis but they do suppress symptoms. The majority of healthcare providers are not aware that birth control pills can cause painful sex and irritative bladder symptoms and that they are a leading cause of Vestibulodynia in premenopausal women.
When people have hormone deficiencies their symptoms feel worse prior to the start of menses. This is because of fluctuating hormones, making deficient urogenital tissues more symptomatic. When people report to a GYN that they feel worse around their period, doctors often think of Endometriosis, therefore it is very important for patients to explain exactly what feels worse or it will be assumed the patient is talking about cramps. Without careful interviewing and adequate knowledge, birth control pills may be prescribed as a solution and really they can be the cause.
Clinical observation has taught us that people with the same set of symptoms will often receive different diagnoses based on the type of physician that they see. If someone with painful sex and urinary urgency and frequency goes to a urologist they will be diagnosed with IC. If they go to a gynecologist they will be diagnosed with Vulvodynia. If they go to both then they think they have multiple diagnoses and that things are really wrong, when in fact many of these symptoms exist together and can be effectively treated by getting to the root cause!
Treatment Considerations and Solutions
We understand the confusion. In today’s world the healthcare system is not effectively taking care of people with symptoms of painful sex and irritative bladder symptoms. There are a handful of doctors in the United States who specialize in these disorders, and an equally small number of excision specialists prepared to treat women with endometriosis. All of these symptoms and diagnoses are also associated with pelvic floor dysfunction, and while the field of pelvic floor physical and occupational therapy is expanding there are certainly more patients than providers. People are misdiagnosed, underdiagnosed, over diagnosed and are suffering as a result.
The first step is identifying the underlying causes of someone’s symptoms. Most women have taken oral contraceptives at some point in their life and a certain percentage of them will have the symptoms of painful sex and irritative bladder symptoms. The urethra is part of the vestibule.
If hormonal deficiencies exist, stopping the cause of hormonal suppression is the first step. The next step is to treat the tissues with various topical hormonal therapies, sometimes systemic support is needed as well. This is true for premenopausal and menopausal women. A pelvic floor physical and occupational therapy examination is also warranted!
For the population of people suffering from severe dysmenorrhea and possibly endometriosis it is recommended to undergo surgery with an excision specialist to confirm or refute the presence of the disease, remove the impaired tissue, and then develop an interdisciplinary treatment plan to tackle co-existing impairments.
Conclusion
Birth control pills can cause painful sex and irritative bladder symptoms in certain women that are genetically predisposed. Birth control pills can suppress dysmenorrhea but this may not make sense if the consequences are to cause other problems. People have been forced to seek out help via social media as many doctors are not aware of these facts, this specialized care is not part of standard medical school curricula, but the landscape is improving as more doctors and physical and occupational therapistss are taking an interest in pelvic health! Hopefully this sheds light onto some of the confusion and provides hope, there is always a solution for these symptoms, people simply need to find the right people to help.
Additional Resources:
Blogs
Do Oral Contraceptive Pills Cause Vulvodynia?
One and Done: The IUD and the Future of Birth Control
Is Your Vagina Healthy? How to Tell Healthy from Unhealthy
Period Health 101: Everything You Should Have Learned in 6th Grade but Didn’t, Part 1 of 3
Vestibulodynia Explained with Follow Up Q&A
YouTube Videos
Top 5 Reasons Your Vulvodynia Symptoms Aren’t Improving
The Truth About The Birth Control Pill
How to Properly Identify Your Vulvodynia & Vestibulodynia
Vulvodynia, Vestibulodynia, Vaginismus…What’s the Difference???
An Introduction to Your Pelvic Floor
Sex Hormones…YES They’re Important!
______________________________________________________________________________________________________________________________________
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
In addition to virtual consultation with our physical and occupational therapistss, we also offer integrative health services with Jandra Mueller, DPT, MS. Jandra is a pelvic floor physical and occupational therapists who also has her Master’s degree in Integrative Health and Nutrition. She offers services such as hormone testing via the DUTCH test, comprehensive stool testing for gastrointestinal health concerns, and integrative health coaching and meal planning. For more information about her services and to schedule, please visit our Integrative Health website page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
FAQ
What are pelvic floor muscles?
The pelvic floor muscles are a group of muscles that run from the coccyx to the pubic bone. They are part of the core, helping to support our entire body as well as providing support for the bowel, bladder and uterus. These muscles help us maintain bowel and bladder control and are involved in sexual pleasure and orgasm. The technical name of the pelvic floor muscles is the Levator Ani muscle group. The pudendal nerve, the levator ani nerve, and branches from the S2 – S4 nerve roots innervate the pelvic floor muscles. They are under voluntary and autonomic control, which is a unique feature only they possess compared to other muscle groups.
What is pelvic floor physical and occupational therapy?
Pelvic floor physical and occupational therapy is a specialized area of physical and occupational therapy. Currently, physical and occupational therapistss need advanced post-graduate education to be able to help people with pelvic floor dysfunction because pelvic floor disorders are not yet being taught in standard physical and occupational therapy curricula. The Pelvic Health and Rehabilitation Center provides extensive training for our staff because we recognize the limitations of physical and occupational therapy education in this unique area.
What happens at pelvic floor therapy?
During an evaluation for pelvic floor dysfunction the physical and occupational therapists will take a detailed history. Following the history the physical and occupational therapists will leave the room to allow the patient to change and drape themselves. The physical and occupational therapists will return to the room and using gloved hands will perform an external and internal manual assessment of the pelvic floor and girdle muscles. The physical and occupational therapists will once again leave the room and allow the patient to dress. Following the manual examination there may also be an examination of strength, motor control, and overall biomechanics and neuromuscular control. The physical and occupational therapists will then communicate the findings to the patient and together with their patient they establish an assessment, short term and long term goals and a treatment plan. Typically people with pelvic floor dysfunction are seen one time per week for one hour for varying amounts of time based on the severity and chronicity of the disease. A home exercise program will be established and the physical and occupational therapists will help coordinate other providers on the treatment team. Typically patients are seen for 3 months to a year.
What is pudendal neuralgia and how is it treated?
Pudendal Neuralgia is a clinical diagnosis that means pain in the sensory distribution of the pudendal nerve. The pudendal nerve is a mixed nerve that exits the S2 – S4 sacral nerve roots, we have a right and left pudendal nerve and each side has three main trunks: the dorsal branch, the perineal branch, and the inferior rectal branch. The branches supply sensation to the clitoris/penis, labia/scrotum, perineum, anus, the distal ⅓ of the urethra and rectum, and the vulva and vestibule. The nerve branches also control the pelvic floor muscles. The pudendal nerve follows a tortuous path through the pelvic floor and girdle, leaving it vulnerable to compression and tension injuries at various points along its path.
Pudendal Neuralgia occurs when the nerve is unable to slide, glide and move normally and as a result, people experience pain in some or all of the above-mentioned areas. Pelvic floor physical and occupational therapy plays a crucial role in identifying the mechanical impairments that are affecting the nerve. The physical and occupational therapy treatment plan is designed to restore normal neural function. Patients with pudendal neuralgia require pelvic floor physical and occupational therapy and may also benefit from medical management that includes pharmaceuticals and procedures such as pudendal nerve blocks or botox injections.
What is interstitial cystitis and how is it treated?
Interstitial Cystitis is a clinical diagnosis characterized by irritative bladder symptoms such as urinary urgency, frequency, and hesitancy in the absence of infection. Research has shown the majority of patients who meet the clinical definition have pelvic floor dysfunction and myalgia. Therefore, the American Urologic Association recommends pelvic floor physical and occupational therapy as first-line treatment for Interstitial Cystitis. Patients will benefit from pelvic floor physical and occupational therapy and may also benefit from pharmacologic management or medical procedures such as bladder instillations.
Who is the Pelvic Health and Rehabilitation Team?
The Pelvic Health and Rehabilitation Center was founded by Elizabeth Akincilar and Stephanie Prendergast in 2006, they have been treating people with pelvic floor disorders since 2001. They were trained and mentored by a medical doctor and quickly became experts in treating pelvic floor disorders. They began creating courses and sharing their knowledge around the world. They expanded to 11 locations in the United States and developed a residency style training program for their employees with ongoing weekly mentoring. The physical and occupational therapistss who work at PHRC have undergone more training than the majority of pelvic floor physical and occupational therapistss and as a result offer efficient and high quality care.
How many years of experience do we have?
Stephanie and Liz have 24 years of experience and help each and every team member become an expert in the field through their training and mentoring program.
Why PHRC versus anyone else?
PHRC is unique because of the specific focus on pelvic floor disorders and the leadership at our company. We are constantly lecturing, teaching, and staying ahead of the curve with our connections to medical experts and emerging experts. As a result, we are able to efficiently and effectively help our patients restore their pelvic health.
Do we treat men for pelvic floor therapy?
The Pelvic Health and Rehabilitation Center is unique in that the Cofounders have always treated people of all genders and therefore have trained the team members and staff the same way. Many pelvic floor physical and occupational therapistss focus solely on people with vulvas, this is not the case here.
Do I need pelvic floor therapy forever?
The majority of people with pelvic floor dysfunction will undergo pelvic floor physical and occupational therapy for a set amount of time based on their goals. Every 6 -8 weeks goals will be re-established based on the physical improvements and remaining physical impairments. Most patients will achieve their goals in 3 – 6 months. If there are complicating medical or untreated comorbidities some patients will be in therapy longer.