By Jandra Mueller, DPT, MS, PHRC Encinitas
September is Interstitial Cystitis/Bladder Pain Syndrome (IC/BPS) Awareness Month!
This diagnosis deserves attention! Interstitial Cystitis/Bladder Pain Syndrome (IC/BPS), is a chronic pelvic pain condition affecting an estimated 12 million people in the United States, and a diagnosis that we see all too often. Despite its prevalence, the causes of Interstitial Cystitis/Bladder Pain Syndrome are multifaceted, and the general lack of knowledge about this condition and the potential causes makes navigating this diagnosis challenging. Despite these challenges, there are treatments available that can provide relief for those suffering!
Interstitial Cystitis/Bladder Pain Syndrome is defined as
“An unpleasant sensation (pain, pressure, discomfort) perceived to be related to the urinary bladder, associated with lower urinary tract symptoms of more than six weeks duration, in the absence of infection or other identifiable causes.”
Over the years, this diagnosis has changed dramatically – from how it is defined to approaching treatment. What was once thought to be an issue with the lining of the bladder, has now expanded to include nine phenotypes. Most people diagnosed with Interstitial Cystitis/Bladder Pain Syndrome are diagnosed based on symptoms alone without a proper workup from a provider to find the root cause, aside from possibly ruling out an infection. The problem with this is that many providers will still treat Interstitial Cystitis/Bladder Pain Syndrome assuming the bladder is the cause, which may not improve symptoms at all, and potentially lead to unwanted side effects. These can range from mild discomfort, pelvic pain, severe pain and more.

Jill Osborne, founder of the Interstitial Cystitis Network has a website www.ic-network.com dedicated to helping individuals understand and navigate this diagnosis. Patients have often found us through her website, and I particularly love how she has outlined the information about this diagnosis, which I will summarize below.
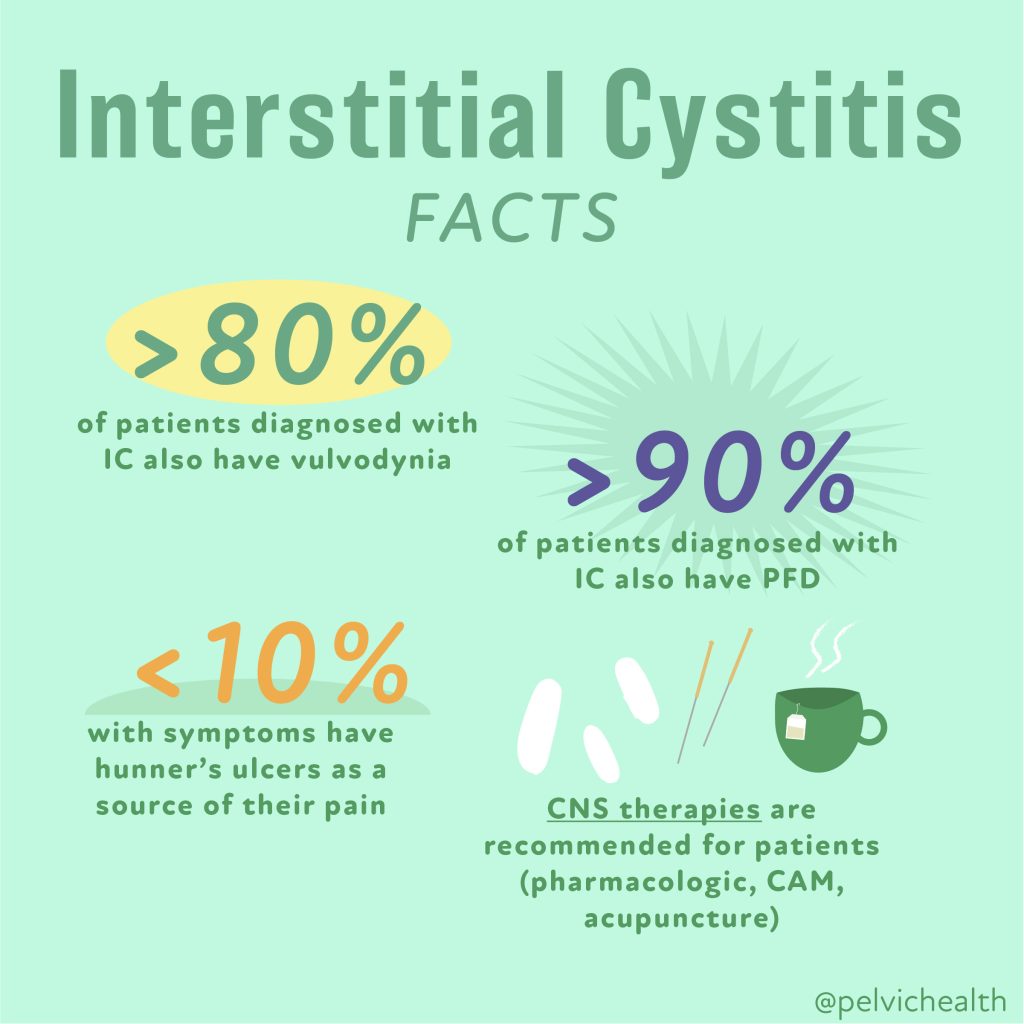
Many providers may not be familiar with the various subtyping, and there are different classifications that can be found online. Sometimes Interstitial Cystitis/Bladder Pain Syndrome is simply classified as Hunner’s lesions (5-10% of cases) and non-ulcerative Interstitial Cystitis/Bladder Pain Syndrome (the remaining 90% of cases). The AUA updated their guidelines in 2022 defining the diagnosis as primarily a neuromuscular disorder rather than a bladder disease. Five subgroups were used to describe the diagnosis and classification to help navigate appropriate treatments, and in 2022 there was further expansion into nine distinct phenotypes to further improve treatment approaches. These phenotypes include:

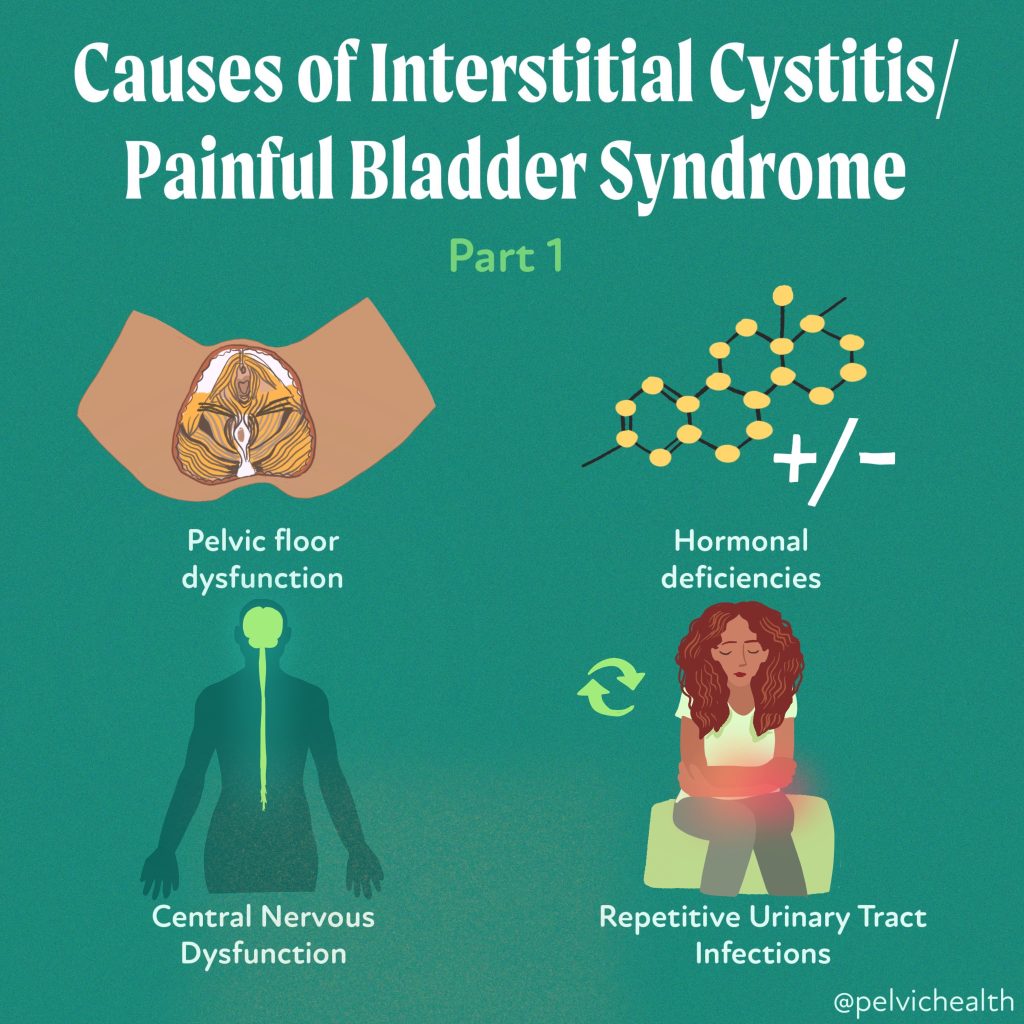
Pelvic Floor Dysfunction (PFD):
One of the most common causes of Interstitial Cystitis/Bladder Pain Syndrome is pelvic floor dysfunction. Studies show that up to 92% of people with Interstitial Cystitis/Bladder Pain Syndrome experience this issue, leading to the American Urological Association recognizing it as a subset (phenotype) of Interstitial Cystitis in 2022. Often characterized by tight or tender pelvic floor muscles, the majority of people with this diagnosis present with Pelvic Floor Dysfunction tenderness and it is imperative to treat the pelvic floor muscles.
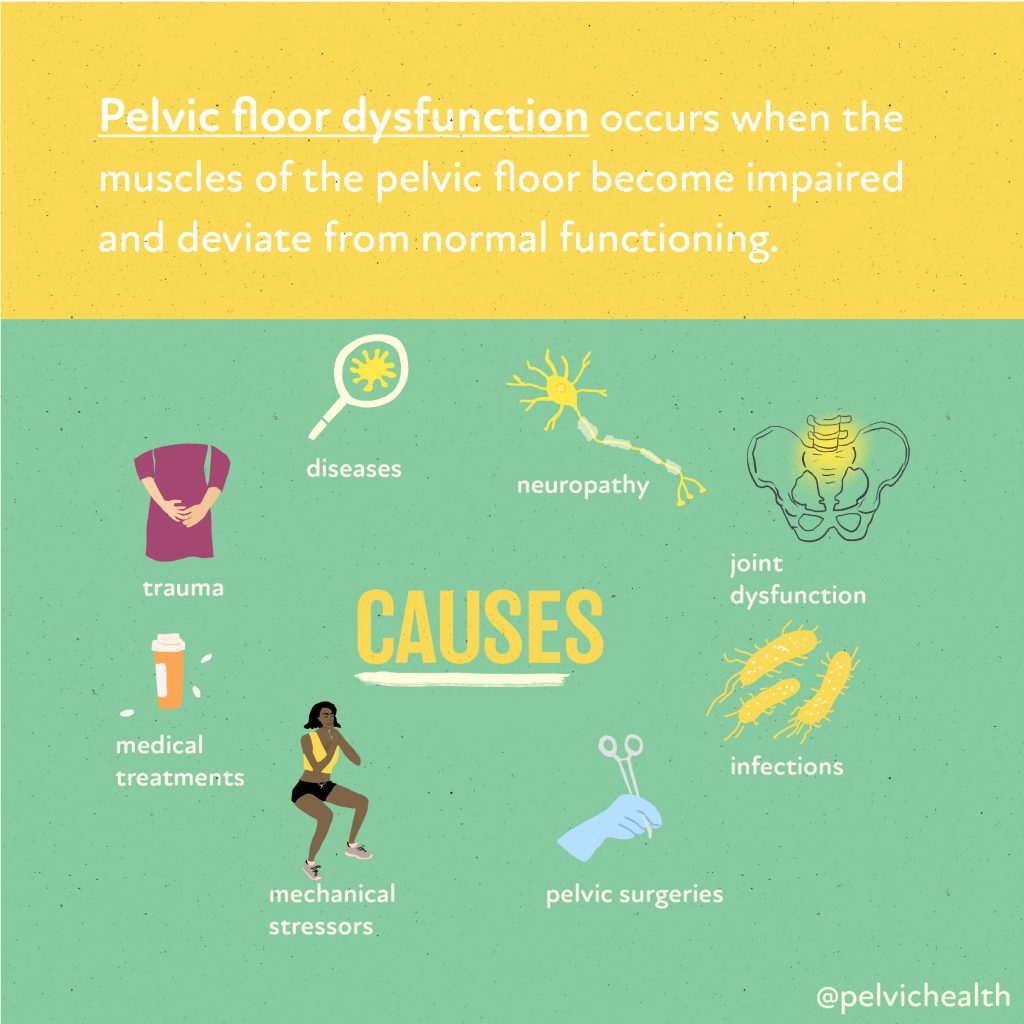
The pelvic floor muscles may be a cause of the symptoms, or may be a secondary finding due to prolonged symptoms and can play a role in maintaining these symptoms. The AUA guidelines recommend pelvic floor physical and occupational therapy as a first-line therapy for this with Interstitial Cystitis/Bladder Pain Syndrome due to the significant overlap and involvement. If you have been given a diagnosis, please consult with a pelvic floor physical and occupational therapists who specializes in sexual medicine and chronic pain conditions. 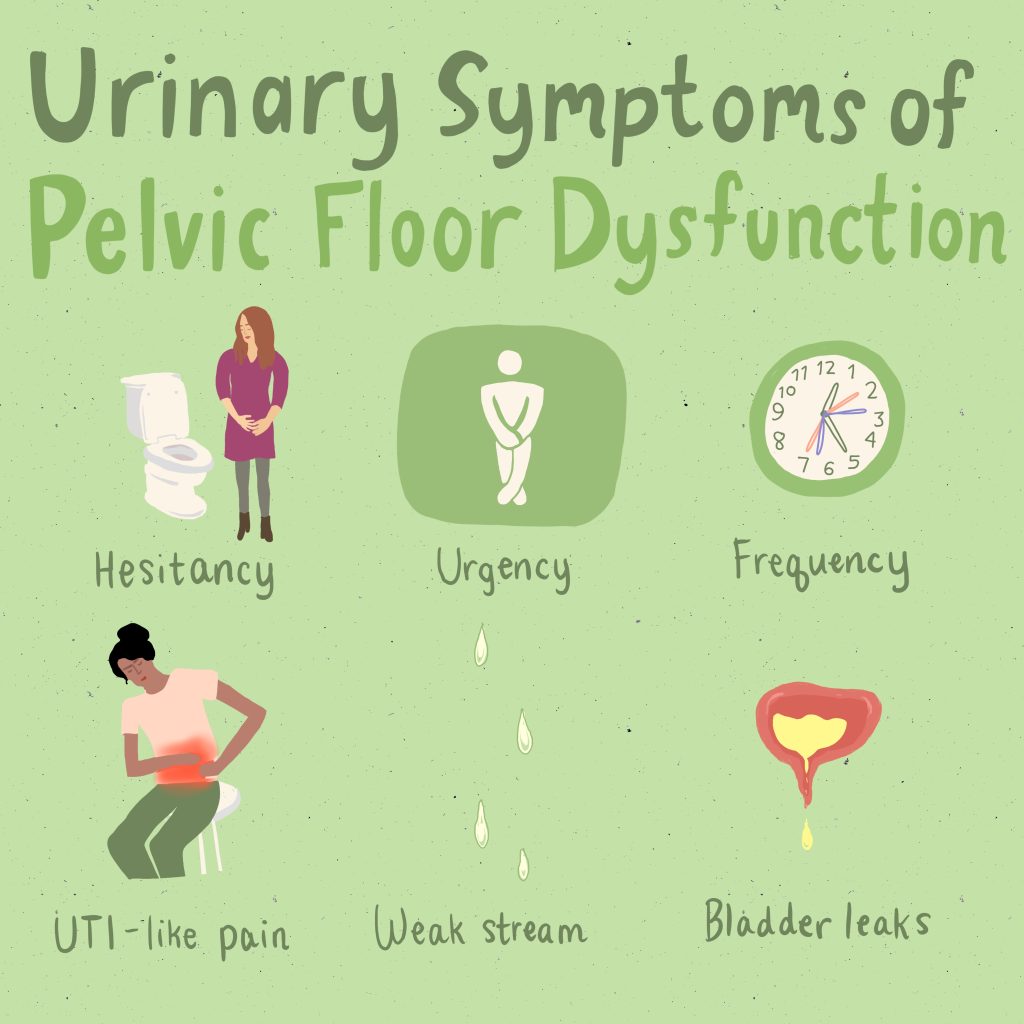
Hunner’s Lesion or Ulcerative IC also referred to as ‘Inflammatory Interstitial Cystitis/Bladder Pain Syndrome:
Bladder inflammation with distinct lesions. These lesions gave name to the diagnosis of “Interstitial Cystitis.” Despite the immense prevalence of these symptoms and the diagnosis of Interstitial Cystitis/Bladder Pain Syndrome, only a small percentage of individuals have these lesions – approximately 5-10%. While some patients do present with Hunner’s lesions, historically these have not always been problematic or symptom producing. Typically treatments involve bladder instillations by a urologist.
Infection-Mediated Interstitial Cystitis/Bladder Pain Syndrome:
Some people do have symptoms that persist after a series of actual urinary tract infections (UTIs), this subtype is new in that after the infection is cleared, the bladder is now hypersensitive. Online forums also talk about possible embedded infections. Treatments when this is suspected include antibiotics directly into the bladder via bladder instillations. Additionally, newer tests such as MicroGenDX labs as well as others, may provide some benefit in identifying pathogens that typical labs do not pick up because of newer testing methods, also offering information on antibiotic resistance which may be a valuable tool if you do in fact suffer from recurring infections.
Neurogenic hypersensitivity Interstitial Cystitis/Bladder Pain Syndrome:
People with these symptoms who do not fit other subtypes but also present with or have diagnoses of Irritable Bowel Syndrome (IBS) or Fibromyalgia. The symptoms are thought to be mediated by the central nervous system and treatments are aimed at calming down the nervous system thus reducing pain. Conservative approaches such as meditation and mindfulness may be suggested along with medications such as low dose antidepressants (which are used off label for these conditions). Additionally, some providers may also recommend instillations in addition to these other therapies.
Multiple Allergies Interstitial Cystitis/Bladder Pain Syndrome:
Histamine and mast-cell mediated issues may be a significant contributor to these symptoms especially if you suffer from other systemic issues such as asthma, chronic rhinitis, skin sensitivities and food allergies. These individuals will likely do the best with addressing the systemic causes and likely respond best to dietary changes minimizing histamine rich foods and the use of antihistamines.
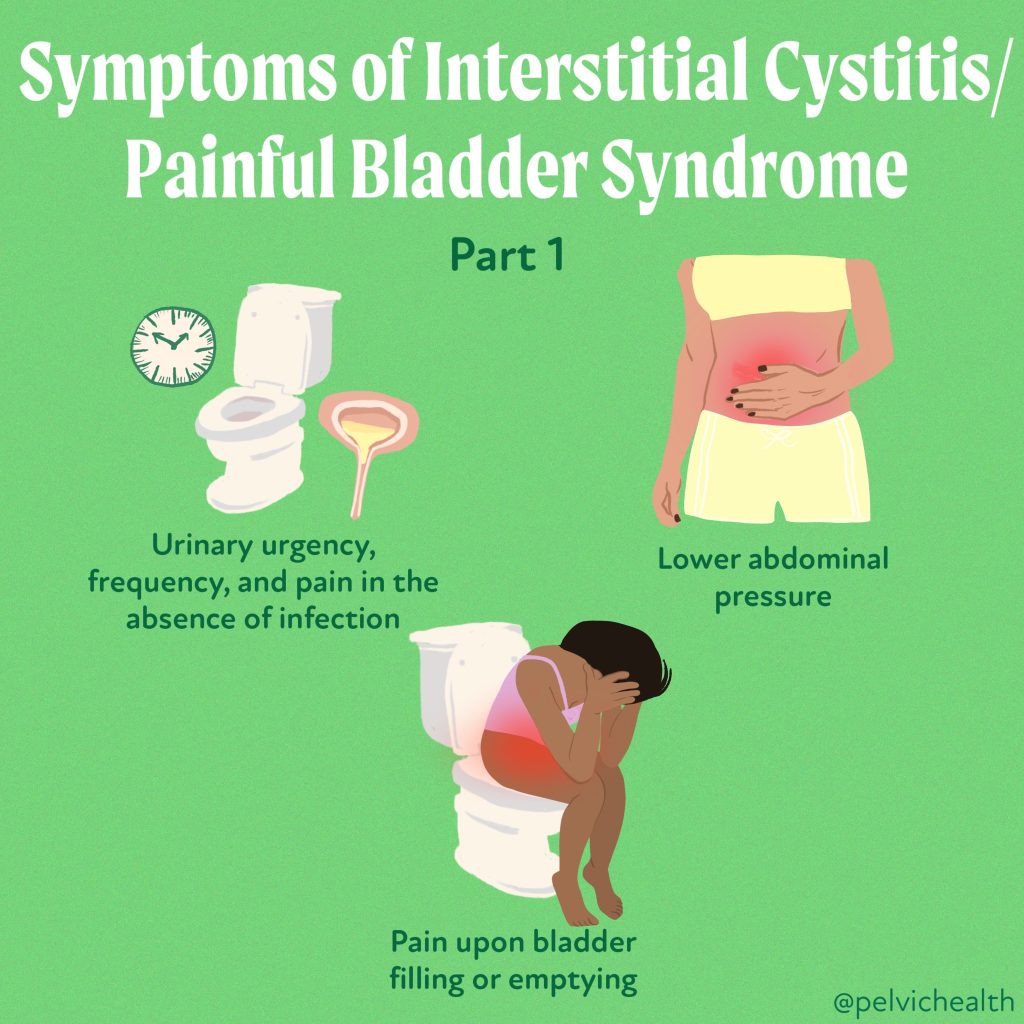
Primary Storage Symptom Syndrome:
This subtype describes those with symptoms related to bladder filling causing them to use the bathroom excessively to avoid bladder distention. Certain medications may be recommended including botox, but these individuals also may respond well to bladder retraining, a tool used by pelvic floor physical and occupational therapistss that work with this population.
Urethral Pain Syndrome:
Another new subtype, not related directly to the bladder is symptoms related or felt in the urethra. This subtype may also be tied into pelvic floor dysfunction or have a hormonal contribution thus the recommendation of a vaginal estrogen. Hormones may be important to address especially if you are going into perimenopause/menopause are post-menopausal, are breastfeeding, have been on oral contraceptive pills, or other medications related to altering hormonal status (such as medications used for breast cancer or endometriosis, etc.) and are experiencing these symptoms.
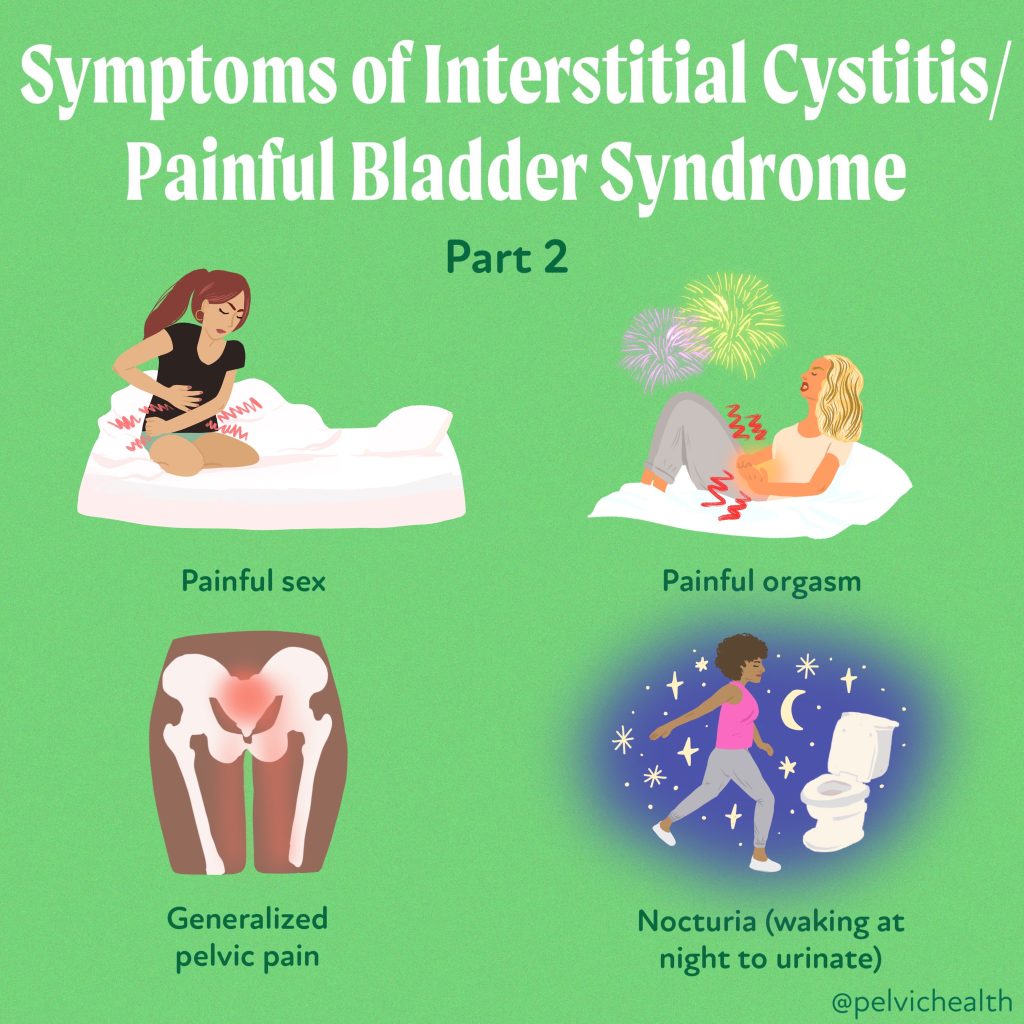
Associated Sexual Pain:
In those experiencing pain with intimacy or having flares of “Interstitial Cystitis/Bladder Pain Syndrome” during or after intimacy, the treatments will be dependent upon where the pain is located. This is not entirely different from previously mentioned subtypes however. For example, the friction of penetrative intercourse may irritate the tissue around the urethra because of lack of adequate hormones – either age related or secondary to certain medications. Additionally, there may be unaddressed pelvic floor dysfunction causing spasms in specific muscles that are causing these symptoms. Treatments will often include pelvic floor physical and occupational therapy as well as hormones and sometimes lidocaine may be recommended for symptom relief.
Interstitial Cystitis Flares:
In those who have had their symptoms under control and then experience a sudden worsening of symptoms such as diet, menstruation, stress, inflection, etc. may need to reassess if the original cause of their symptoms remains the cause of their flare, or may need to consider reassessing how they approach treatment if their normal tools and treatments aren’t working.
While these subgroups help to better understand where the pain is coming from in order to approach treatment, a thorough workup is still needed to best understand the factors contributing to symptoms in each individual case. Despite the daunting nature of this diagnosis, we have learned so much about the causes of these symptoms and how to approach treatment.
Real life success story!
A patient I have been working with recently was diagnosed with interstitial cystitis/bladder pain syndrome in her early 30’s, she was prescribed Elmiron (a medication commonly used to treat Hunner’s lesion subtype) and this worked for her for many years and was under control with minimal to no symptoms.
In her late 40’s, she had what she describes as a flare up and none of the tools she had previously used were working. During our evaluation, she reported that just before her flare, she noticed that her menstrual cycle was beginning to change, was becoming more painful and her provider suggested she start on oral contraceptive pills to reduce her menstrual pain, and was likely perimenopausal. Shortly after, her IC flares began.
Upon examination, she had signs and symptoms consistent with Vestibulodynia, or more accurately, Genitourinary Syndrome of Menopause along with tight and painful pelvic floor muscles. In addition to pelvic floor physical and occupational therapy, she was referred to a urologist specializing in sexual medicine. She stopped her oral contraceptives and began using a topical hormonal cream to address the tissue irritation along with systemic hormones. Not too long after starting this regimen, her flares began to subside.
She has now had minimal to no symptoms for several months, and is completely off her Elmiron!
Vestibulodynia
Do you know the difference between Vulvodynia & Vestibulodynia? Vulvodynia simply means pain in the vulva, which includes the clitoris, labia, mons pubis, perineum, hymen, and vestibule
Vestibulodynia is pain in the vestibule, a more precise description for the area of pain. The vestibule is depicted in the picture above and extends from inside the labia minora to the hymen & houses the opening of the urethra and our major & minor glands that provide some of our lubrication when we are aroused.⠀
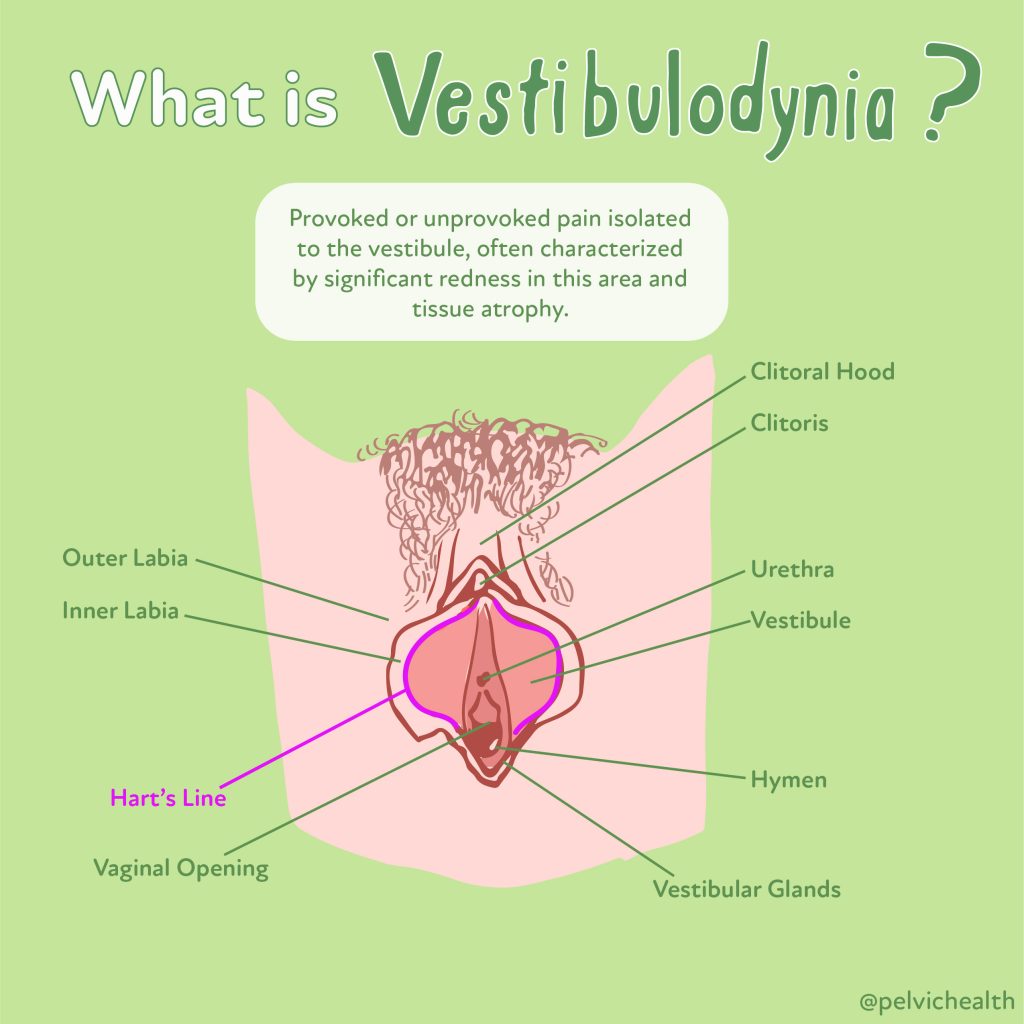
Understandably, most people with painful sex & vulvar pain may not know where the vestibule is unless they have seen vulvar expert who explains the differences. Importantly, the vestibule is anatomically different from the rest of the vulva.⠀
Genitourinary Syndrome of Menopause
As people age, circulating hormones decline and pelvic floor dysfunction rises. The combination of these changes can cause unnecessary suffering and distress. The unfortunate news is that most people do not realize their symptoms may be related to hormonal deficiencies & musculoskeletal issues, the good news is both scenarios are treatable!
Perimenopause begins in the 40s for most people. Symptoms of the Genitourinary Syndrome of Menopause (GSM) can start around this time period, before hot flashes and other common systemic menopause symptoms. For others, symptoms may start later but if left untreated most menopausal people will experience GSM.
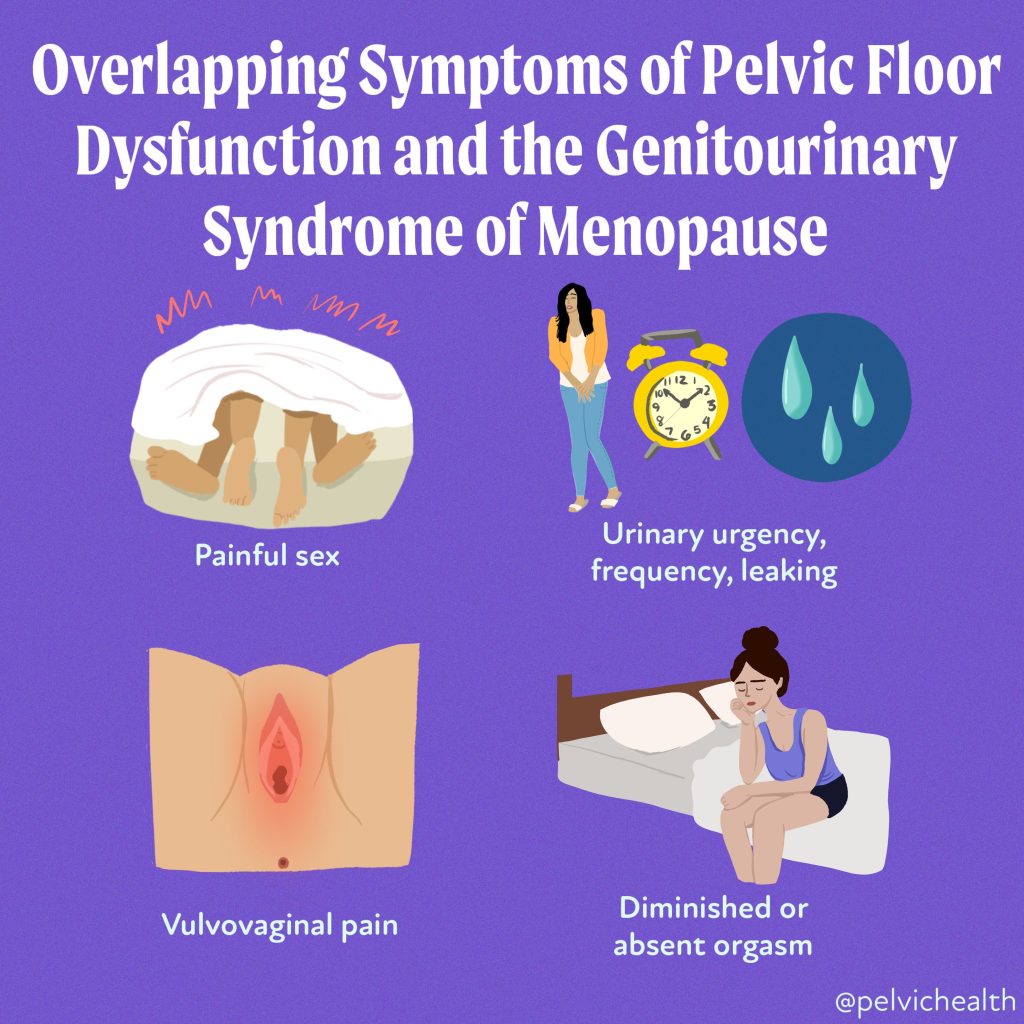
Experts recommend local hormone therapy directly to the vulva and vagina to reduce vaginal dryness, painful sex, diminished orgasm, irritative bladder symptoms and recurrent UTIs. Systemic hormone therapy is different from vaginal hormone therapy + we recommend speaking with providers that follow the North American Menopause Society Guidelines to help people manage their genitourinary symptoms.
The symptoms of Pelvic Floor Dysfunction mimic Genitourinary Syndrome of Menopause (GSM) symptoms. When pelvic floor muscles become tight they cause painful sex, urinary urgency/frequency and pain. If the PF muscles are weak people may experience urinary/fecal leaking, pelvic and bladder pressure, and pelvic organ prolapse.
Many people may have muscles that are tight in some areas and weak in others, both are problematic situations because the pelvic floor needs to function as part of our core. Without proper neuromuscular function people can also experience hip, low back and pelvic girdle pain. We recommend all entering perimenopause and menopause undergo a pelvic floor evaluation to best optimize their pelvic health!
The combination of proper HT and PFPT can be a game changer for people during this phase of life!
Interstitial Cystitis/Bladder Pain Syndrome Do’s and Don’ts
Interstitial Cystitis/Bladder Pain Syndrome may seem overwhelming due to its wide range of symptoms and causes, the condition is manageable with proper treatment. Identifying the underlying causes—whether it’s pelvic floor dysfunction, hormonal imbalances, or a combination of factors —allows for tailored therapeutic approaches. For anyone experiencing any of the symptoms above, it’s important to seek help from a qualified medical provider and begin appropriate treatment.
How we can help you
If you’re experiencing sexual function issues, it’s important to see a therapist for pelvic floor therapy. Before coming in, you can always take advantage of Telehealth through technologies, such as computers and mobile devices, to access healthcare services remotely and manage your health care. This approach allows patients to receive care and consultation from the comfort of their homes.
After a virtual consultation, you can then follow whatever the health professional suggests. When you are advised to go to a clinic, they will evaluate your pelvic floor to determine if it’s contributing to your symptoms. The physical and occupational therapists will discuss your medical history, previous diagnoses, and treatments you’ve tried, as well as their effectiveness. We understand what you’re going through and many people come to us feeling frustrated.
Learn more and request a virtual appointment via our IC page.
Resources
Media
Check out PHRC Cofounder Stephanie Prendergast on Bustle about pelvic floor physical and occupational therapy & IC!
The Interstitial Cystitis Association and the Interstitial Cystitis Network are two patient advocacy groups working hard to raise awareness about IC/PBS and help patients through the diagnosis and treatment process.
Book
We LOVE Nicole Cozean’s book, The Interstitial Cystitis Solution! Stay tuned to our YouTube Channel, Stephanie is interviewing Nicole later this month, diving deeper about multi-faceted and effective treatment plans for people recovering from IC.
Blog Posts
The Most Proven IC Treatment: Pelvic Floor Physical and Occupational Therapy
Causes of Interstitial Cystitis/Painful Bladder Syndrome
Latchkey Incontinence; What is It and How Does PFPT Help? Part 1
Can TMS help people with Interstitial Cystitis/Painful Bladder Syndrome?
Patient Success Stories
For more success stories, check out our book Pelvic Pain Explained!
How to find informed medical providers
International Pelvic Pain Society Find a Provider
American Physical and Occupational Therapy Association’s Section on Women’s Health PT Locator
Herman and Wallace Find a Provider
Pelvic Guru Provider Directory
______________________________________________________________________________________________________________________________________
Check out our recently published e-book titled “Vulvodynia, Vestibulodynia, and Vaginismus,” designed to empower and inform individuals on their journey towards healing and understanding.
Did you know we opened our 11th location in Columbus, OH? Now scheduling new patients- call (510) 922-9836 to book!
Are you unable to come see us in person in the Bay Area, Southern California or New England? We offer virtual physical and occupational therapy appointments too!
Virtual sessions are available with PHRC pelvic floor physical and occupational therapistss via our video platform, Zoom, or via phone. For more information and to schedule, please visit our digital healthcare page.
Do you enjoy or blog and want more content from PHRC? Please head over to social media!
Facebook, YouTube Channel, Twitter, Instagram, Tik Tok